
The burgeoning market for obesity treatments, propelled recently by the widespread adoption of GLP-1 receptor agonists, stands at a critical juncture. While these medications have undeniably transformed the landscape for many, a growing chorus of scientific and industry voices, including Mark Bagnall, CEO of Phenomix Sciences, warns against the perils of overconfidence in a "one-treatment-for-all" narrative. Bagnall draws a parallel to the early days of the internet, recalling how it was once touted as a universal panacea only to reveal its own complexities. This analogy underscores a fundamental truth emerging in obesity care: effective, sustainable solutions demand a more nuanced, personalized approach, akin to the precision medicine revolution reshaping oncology.
The Rise and Rethink of GLP-1s in the Trillion-Dollar Market
The global obesity market has witnessed unprecedented growth, reaching an estimated value that propelled Eli Lilly to become the first pharmaceutical company to surpass a $1 trillion market capitalization. This monumental achievement, realized in late 2025, was largely fueled by the surging global demand for its highly effective obesity medications, particularly tirzepatide (marketed as Mounjaro for diabetes and Zepbound for weight loss) and semaglutide (Ozempic for diabetes, Wegovy for weight loss, produced by Novo Nordisk). These GLP-1 receptor agonists mimic the action of glucagon-like peptide-1, a hormone that regulates appetite and insulin secretion, leading to significant weight loss for many users. By 2025, over 30 million Americans were reportedly utilizing GLP-1 medications for weight management, a testament to their profound impact.
The marketing surrounding these drugs has often presented them as a definitive, almost miraculous, solution for obesity, a condition affecting over 40% of American adults and presenting a significant global health crisis. The World Health Organization (WHO) estimates that global obesity rates have nearly tripled since 1975, leading to a cascade of related health issues including type 2 diabetes, cardiovascular diseases, certain cancers, and musculoskeletal disorders. The economic burden of obesity is staggering, encompassing direct healthcare costs and indirect costs from lost productivity. Given this immense challenge, the arrival of potent pharmacotherapies like GLP-1s was met with understandable enthusiasm.
However, a recent survey conducted by Phenomix Sciences revealed a disconnect between public perception and patient experience. Despite the pervasive marketing, only 33% of patients surveyed genuinely viewed GLP-1s as a definitive solution for their obesity. This statistic hints at the limitations and complexities that extend beyond the initial promise.
Industry Insiders Signal a Shift: Beyond the "Silver Bullet"
The pharmaceutical industry itself, often perceived as the primary driver of the GLP-1 boom, appears to be hedging its bets. Mark Bagnall points to the sheer volume of drugs currently in development as compelling evidence that even drug companies do not consider GLP-1s to be the ultimate "panacea." As of 2025, TD Cowen reported over 160 obesity drugs in various stages of development, exploring a remarkable 68 different mechanisms of action. By early 2026, this number had reportedly climbed to over 200 new drugs, some of which are variations of GLP-1s, but many others employ entirely different pharmacological pathways. This robust pipeline signals a clear understanding within the industry that a diverse array of solutions will be essential to effectively tackle the multifaceted challenge of obesity.
Even the World Health Organization, while acknowledging the utility of GLP-1s, frames them within a broader, more comprehensive public health strategy. In December 2025, the WHO issued a conditional recommendation for GLP-1 therapies, explicitly stating that they should be integrated into a holistic approach. This comprehensive strategy, as outlined by the organization, mandates adherence to healthy diets, engagement in regular physical activity, and sustained support from healthcare professionals. The WHO Director-General underscored this perspective, declaring unequivocally that "medication alone won’t solve this global health crisis." This official stance further reinforces the growing consensus that GLP-1s, while powerful tools, represent only one piece of a much larger, intricate puzzle.
The Unveiled Realities: Side Effects and Patient Dissatisfaction
While the efficacy of GLP-1s in promoting weight loss is well-documented, the experience of patients is not uniformly positive, largely due to the prevalence of side effects. The most common adverse events are transient gastrointestinal issues such as nausea, vomiting, diarrhea, and constipation. However, more significant concerns have emerged, particularly regarding the potential for muscle and bone density loss. An October 2024 review published by the American Heart Association (AHA) cited two studies indicating that less than half of the total weight lost with GLP-1 medications originated from fat tissue, with a substantial portion attributed to the reduction of lean muscle mass.
The implications of muscle mass loss are far-reaching. Muscle tissue is crucial for metabolic health, strength, mobility, and overall vitality. For older patients or those already predisposed to weakness, significant muscle loss can introduce a new category of health risks, including increased susceptibility to falls and bone fractures. Bagnall highlights this concern: "You have to be really thoughtful, because there is a general health benefit to muscle mass – but at some point, if you’re already weak and older, now we go into a whole other category of issues: falls, broken bones."
Compounding these medical concerns are the financial and emotional burdens on patients. The Phenomix survey revealed a worrying gap in patient education, with only 45% of users fully aware of the potential risks associated with GLP-1s, and a significant 17% entirely unaware. Patients are often compelled to pay substantial out-of-pocket expenses for these medications, which can run into hundreds or even thousands of dollars monthly, especially when insurance coverage is lacking or restrictive. Furthermore, Bagnall notes that patients may incur an additional $1,000 or more out of pocket to manage side effects, adding another layer of financial strain to an already costly treatment regimen.
While many experience only transient side effects, for a subset of patients, these adverse reactions can be persistent or severe, ultimately leading to discontinuation of the medication. This outcome can be particularly disheartening. "They’ve been told there’s a silver bullet. And then six months later, nothing happened," Bagnall laments. "I think where you really feel despair as a patient is when the thing that has been promised to you as the answer to your problems fails." This sentiment underscores the critical need for more personalized therapeutic strategies that account for individual patient responses and vulnerabilities.
The Dawn of Precision Medicine: Tailoring Treatment to the Individual
The variability in patient response to GLP-1s, both in terms of efficacy and side effects, strongly suggests underlying biological differences. Bagnall posits that genetic variations likely play a significant role in determining how individuals metabolize and react to these medications. This insight forms the bedrock of Phenomix Sciences’ innovative approach: leveraging genetic testing to identify which patients are most likely to benefit from GLP-1s and, critically, which individuals may be intolerant due to severe or permanent side effects.
Phenomix’s philosophy is rooted in groundbreaking research conducted at the Mayo Clinic, which identified four distinct obesity subtypes, or "phenotypes": "hungry brain," "hungry gut," "emotional hunger," and "slow burn." These phenotypes are not merely descriptive labels but represent specific dysregulations within the complex gut-brain axis, governing how signals of hunger and fullness are communicated between the digestive system and the brain.
- Hungry Brain: Patients with this phenotype exhibit an overactive appetite drive originating in the brain.
- Hungry Gut: Characterized by impaired satiety signals from the gut, leading to persistent feelings of hunger.
- Emotional Hunger: Driven by psychological factors, where eating is triggered by stress, anxiety, or other emotional states rather than physiological need.
- Slow Burn: Defined by a lower resting metabolic rate, meaning the body burns fewer calories at rest.
Crucially, patients respond differently to various obesity treatments based on their specific phenotype. For instance, individuals identified with the "hungry brain" phenotype have demonstrated favorable responses to medications like phentermine or topiramate extended release (e.g., Qsymia). Patients experiencing "emotional hunger" often find greater success with drugs such as Contrave (naltrexone/bupropion). Conversely, those with the "hungry gut" phenotype are typically the best responders to GLP-1 receptor agonists, indicating that these drugs are indeed highly effective, but for a specific subgroup of the obese population.
This phenotypic stratification offers a powerful alternative to the "trial-and-error" approach that often characterizes current obesity management. Bagnall highlights that even older drugs, which might offer an average weight loss of around 10% across the general obese population, can achieve comparable efficacy to GLP-1s (up to 17% weight loss) when precisely matched to the appropriate "hungry brain" patient. This demonstrates that the issue isn’t necessarily the efficacy of older drugs, but rather the lack of tools to identify the right patient for them. Genetics, according to Bagnall, can explain a remarkable 70% to 80% of a patient’s individual response to obesity medications, underscoring the immense potential of a precision medicine framework.
Phenomix Sciences: Pioneering the MyPhenome Test

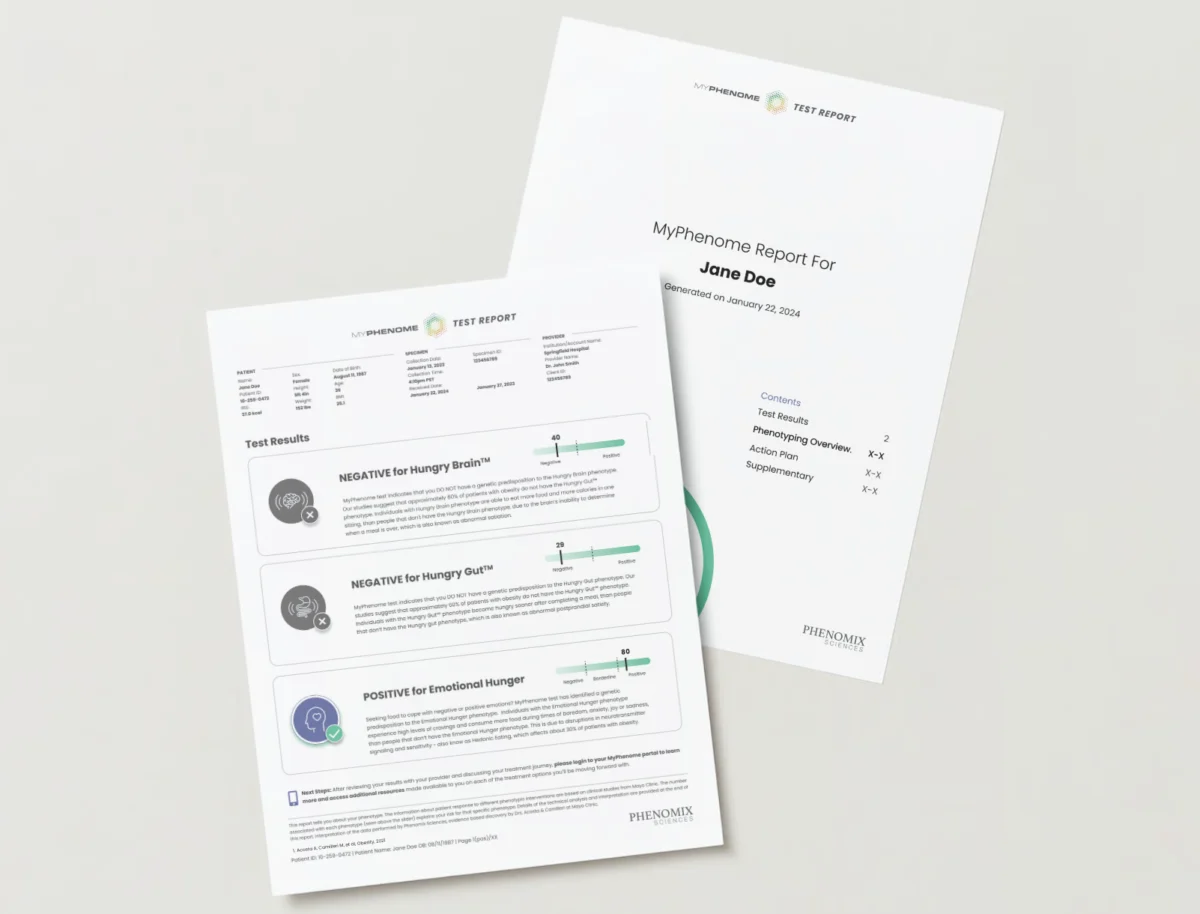
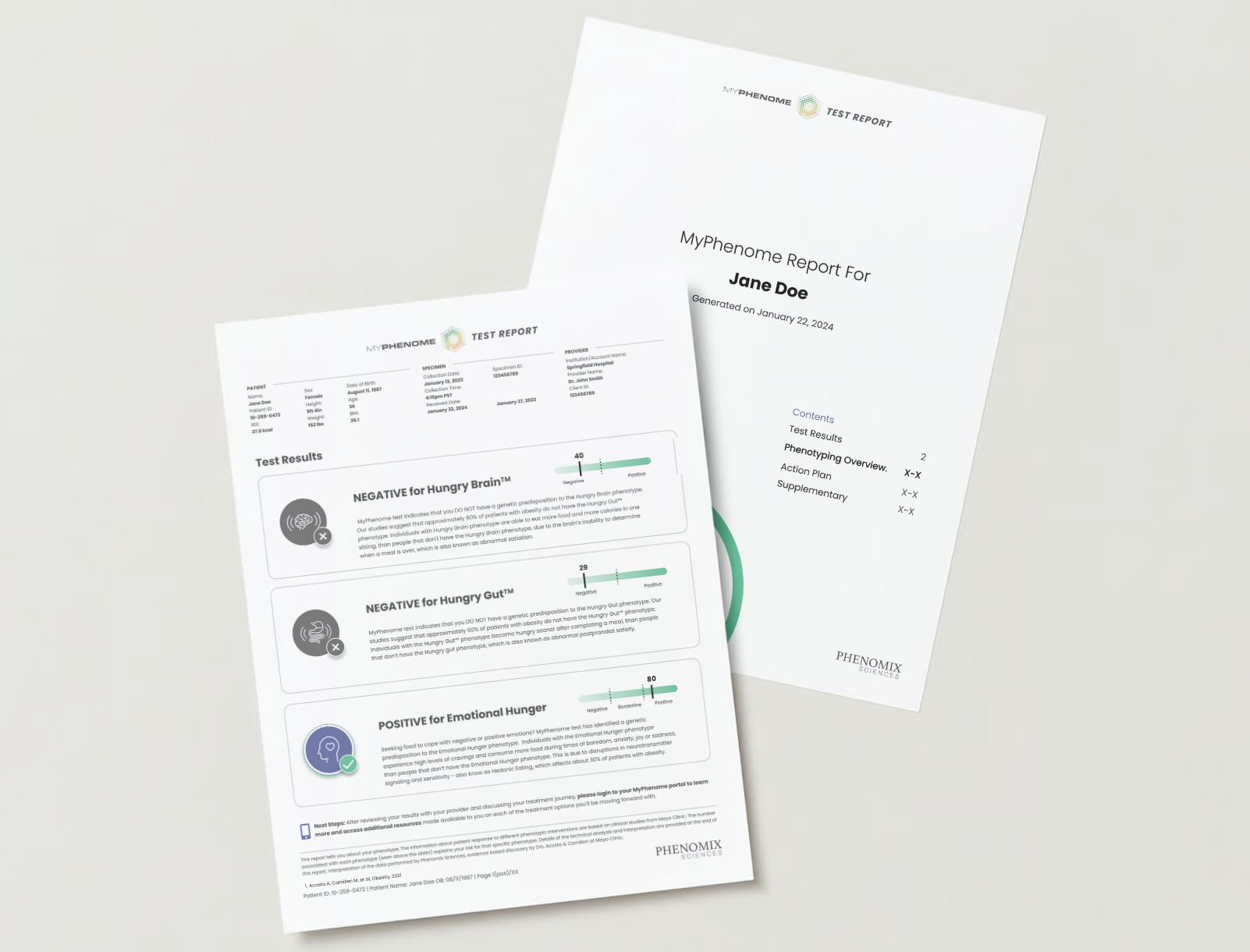
Phenomix Sciences is actively developing its MyPhenome test, a diagnostic tool designed to characterize an individual’s specific obesity phenotype and predict their response to various medications, including GLP-1s. A key objective of this test is to identify "super intolerant" patients—those who are genetically predisposed to experiencing severe, permanent nausea or vomiting when taking GLP-1s. By identifying these individuals before treatment initiation, the MyPhenome test could prevent immense patient suffering, unnecessary healthcare costs, and the despair associated with failed therapies.
The MyPhenome test aims to provide clinicians with actionable insights, allowing them to prescribe the most effective medication for each patient from the outset, rather than relying on a generalized approach. The example report from the MyPhenome test visually demonstrates how patients could receive personalized recommendations, moving obesity treatment from a broad-stroke strategy to a highly targeted intervention. "To be able to come in and provide a solution, that feels pretty good to us," Bagnall expresses, articulating the company’s commitment to improving patient outcomes and satisfaction.
Economic and Healthcare Implications: A Transformative Shift
The shift towards precision medicine in obesity carries profound implications for the healthcare system, pharmaceutical market, and patient care. Economically, it promises a more efficient allocation of resources. By reducing the number of patients undergoing ineffective or poorly tolerated treatments, healthcare costs associated with managing side effects, repeated consultations, and switching medications could be significantly lowered. For pharmaceutical companies, it means a refined market segmentation, where the value of their drugs is enhanced by their ability to precisely target the right patient population. This encourages further innovation in drug development, moving beyond broad-spectrum agents towards more specific, mechanism-based therapies.
The adoption of precision medicine also holds the potential to reduce the emotional and financial burden on patients. Fewer failed treatments mean less frustration, less out-of-pocket spending on ineffective drugs or side effect management, and ultimately, a higher likelihood of achieving sustainable weight loss and improved health. This could lead to better adherence to treatment plans and, in turn, a reduction in the long-term complications associated with obesity, such as diabetes and heart disease.
A Vision for the Future: Curing Obesity on a Mass Scale
Mark Bagnall envisions a future where obesity treatment mirrors the sophisticated, individualized approach currently seen in oncology. Cancer treatment has undergone a dramatic transformation from chemotherapy to targeted therapies and immunotherapies, guided by genomic profiling of tumors. Bagnall believes obesity is on a similar trajectory. He predicts that within the next decade, the market will feature upwards of 50 different obesity drugs, each targeting specific metabolic pathways or phenotypes. This expanded pharmacopeia will enable clinicians to select therapies with unprecedented precision, fundamentally changing how obesity is managed.
Looking further ahead, Bagnall makes a bold and optimistic prediction: "In 20 years, we will have cured it." While "cured" in the context of a complex chronic disease like obesity might imply lifelong management rather than eradication, his statement underscores the transformative potential of precision medicine to render obesity a largely manageable, preventable, or even reversible condition for the vast majority of individuals. This vision represents a significant leap from the current landscape, moving beyond the "silver bullet" mentality towards a future where personalized, scientifically informed interventions empower patients and clinicians to effectively tackle one of the greatest global health challenges of our time.











Leave a Reply