
A breakthrough study from the University of Colorado Boulder has identified a specific neural pathway that acts as a gatekeeper for chronic pain, potentially explaining why some temporary injuries evolve into lifelong conditions. The research, published in the Journal of Neuroscience, highlights a previously under-studied region of the brain known as the caudal granular insular cortex (CGIC). By manipulating this circuit in animal models, researchers successfully prevented the development of chronic pain and, perhaps more significantly, reversed persistent pain that had already become established. This discovery offers a new biological roadmap for treating chronic pain without the use of addictive opioids, signaling a paradigm shift in how neurology approaches sensory disorders.
The Biological Architecture of Persistent Pain
Chronic pain is often described as a "maladaptive" response by the nervous system. While acute pain serves as a vital survival mechanism—alerting the body to immediate injury—chronic pain persists long after the initial tissue damage has healed. The University of Colorado Boulder team focused on the transition from the former to the latter, seeking to understand the exact moment the brain decides to keep the "alarm" ringing.
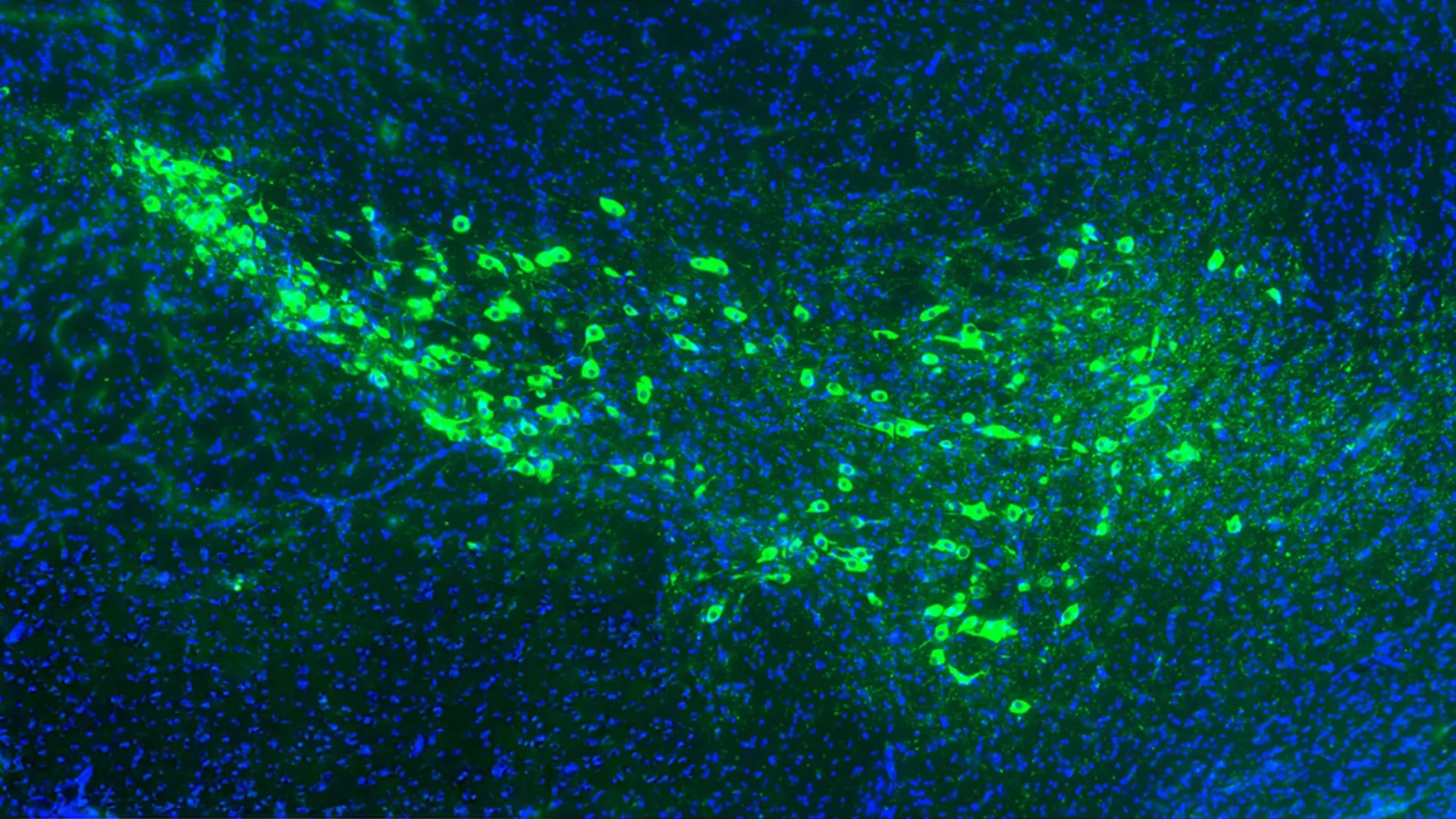
The study centered on the CGIC, a sub-region of the insula located deep within the cerebral cortex. The insula is known to process a wide array of signals, including emotions, taste, and internal bodily sensations. However, the CGIC’s specific role in pain chronicity remained elusive until now. Using advanced neuro-imaging and molecular tracking, the researchers observed that when a nerve is injured, the CGIC becomes hyperactive. This activity does not merely reflect the pain; it actively instructs the rest of the nervous system to remain in a state of high alert.
Senior author Linda Watkins, a distinguished professor of behavioral neuroscience, noted that the CGIC serves as a "decision maker." According to Watkins, the circuit essentially tells the spinal cord to continue transmitting pain signals to the brain, even in the absence of a new injury. When the researchers used "chemogenetic" tools to silence this specific group of neurons, the chronic pain disappeared, effectively "melting away" the persistent discomfort in the animal subjects.
A Decade of Incremental Discovery: The Research Chronology
The identification of the CGIC-driven pathway is the culmination of over a decade of research. To understand the significance of the current findings, it is necessary to look at the timeline of discovery within the Watkins Lab and the broader scientific community.
In 2011, early studies by Watkins and her colleagues first hinted that the insular cortex played a disproportionate role in pain sensitivity. At the time, technology limited the ability of scientists to isolate specific neurons without damaging the surrounding brain tissue. For years, the only way to study the effects of the insula on pain was through lesion studies—physically removing parts of the brain—which provided crude data but offered no viable path for human clinical treatment.
By 2018, the emergence of more sophisticated fluorescent proteins allowed the team to begin mapping the connections between the CGIC and other brain regions with microscopic precision. This led to the discovery that the CGIC does not work in isolation; it forms a critical link in a chain that includes the somatosensory cortex—the area of the brain responsible for processing the physical sensation of touch—and the dorsal horn of the spinal cord.
The current study, published in 2024, represents the final piece of this puzzle. By using Designer Receptors Exclusively Activated by Designer Drugs (DREADDs), the team was able to turn these specific neurons on and off like a light switch. This confirmed that the CGIC is not necessary for the initial sensation of pain but is the primary driver of its long-term persistence.
Supporting Data: The Scale of the Chronic Pain Crisis
The implications of this research are underscored by the staggering statistics regarding chronic pain in the United States. Data from the Centers for Disease Control and Prevention (CDC) indicates that approximately 20.9% of U.S. adults—roughly 51.6 million people—suffer from chronic pain. Furthermore, 6.9% of adults experience "high-impact chronic pain," defined as pain that frequently limits life or work activities.
The economic burden is equally significant. Estimates suggest that chronic pain costs the U.S. economy up to $635 billion annually in medical treatments, disability payments, and lost productivity. This exceeds the annual costs of heart disease ($309 billion) and cancer ($243 billion) combined.
A key feature of many chronic pain conditions is allodynia, where a stimulus that does not normally provoke pain—such as the brush of clothing against the skin—becomes excruciating. The University of Colorado study found that the CGIC-somatosensory pathway is the direct cause of this phenomenon. When the circuit is active, it re-wires the spinal cord’s processing of touch, causing the brain to misinterpret gentle tactile signals as intense pain.
Technical Innovations and the "Gold Rush of Neuroscience"
The study’s first author, Jayson Ball, who recently transitioned from Watkins’ lab to the neural technology firm Neuralink, describes the current era as a "gold rush of neuroscience." This surge in discovery is fueled by tools that allow for cell-specific manipulation.
In this study, the researchers utilized chemogenetics to achieve their results. This process involves:
- Genetic Engineering: Introducing specific genes into the neurons of the CGIC using a viral vector.
- Receptor Expression: These genes cause the neurons to grow unique receptors that do not respond to any natural chemicals in the body.
- Controlled Activation: A synthetic drug, which is otherwise inert, is administered to the subject. This drug binds only to the engineered receptors, allowing the scientists to silence or activate the CGIC neurons at will.
This level of precision is what differentiates modern neuroscience from the pharmacological approaches of the 20th century. While traditional painkillers like opioids flood the entire brain and body with chemicals—leading to side effects like respiratory depression, constipation, and addiction—chemogenetics targets only the "broken" circuit.
Reactions from the Scientific and Medical Communities
While the study was conducted in rats, the medical community has reacted with cautious optimism. Neurologists specializing in pain management point out that the insular cortex in humans is structurally and functionally similar to that of primates and rodents, suggesting a high likelihood that a similar circuit exists in the human brain.
"The identification of a ‘stop button’ for chronic pain in the brain is the holy grail of pain research," said one independent neuroscientist not involved in the study. "If we can translate these findings into human therapies, we could potentially treat conditions like fibromyalgia, complex regional pain syndrome (CRPS), and chronic back pain at their source rather than just masking the symptoms."
Public health officials have also noted the potential impact on the opioid epidemic. Since the late 1990s, the over-prescription of opioid medications for chronic pain has led to a national crisis. If physicians had access to non-addictive, circuit-based therapies, the reliance on narcotics could be drastically reduced.
Broader Impact and Future Implications
The transition of Jayson Ball to Neuralink highlights a burgeoning field where academic research meets private-sector technology: brain-machine interfaces (BMIs). While Ball’s research at CU Boulder utilized chemogenetics, the knowledge of the CGIC pathway could be applied to implanted neural devices.
In the future, patients with intractable chronic pain might receive a small, minimally invasive implant that monitors the CGIC. When the device detects the neural signatures of chronic pain, it could deliver precise electrical pulses to "reset" the circuit, similar to how a pacemaker regulates a heart rhythm.
However, several hurdles remain. Applying these findings to humans requires rigorous clinical trials to ensure safety and efficacy. Scientists must also determine what triggers the CGIC to become hyperactive in the first place. Is it a result of genetic predisposition, the severity of the initial injury, or perhaps psychological factors like stress and trauma?
Conclusion: A New Frontier in Sensory Medicine
The research from the University of Colorado Boulder provides a definitive answer to a question that has plagued medicine for decades: why does pain sometimes refuse to leave? By identifying the CGIC as the brain’s "chronic pain switch," Watkins, Ball, and their team have moved the field closer to a future where long-term suffering is no longer an inevitable consequence of injury.
As neuroscience continues its "gold rush," the focus is shifting away from general brain regions and toward the specific sub-populations of cells that govern our experiences. For the millions of people living with chronic pain, this study represents more than just a scientific milestone; it offers a tangible hope that the "false alarm" in their nervous systems can finally be silenced. Through the integration of genetic engineering, precision medicine, and advanced technology, the medical community is now equipped with the knowledge to potentially turn the tide against one of the most pervasive and costly health challenges of the modern era.











Leave a Reply