Merck has unveiled its investigational KRAS G12C inhibitor, calderasib, positioning it not merely as another potent molecule in a rapidly evolving therapeutic landscape, but as a strategically designed agent optimized for combinability and sustained efficacy against one of oncology’s most formidable targets. This approach marks a significant departure from previous KRAS G12C inhibitors, which often struggled with rapid resistance mechanisms when used as monotherapies. The company’s development philosophy for calderasib emphasizes a biomarker-driven, tumor-agnostic strategy, drawing parallels from its successful precedent with pembrolizumab.
The Elusive KRAS Target: A Decades-Long Challenge in Oncology
The journey to effectively target the KRAS gene represents one of the most compelling sagas in modern oncology. KRAS, an acronym for Kirsten rat sarcoma virus, encodes a critical protein involved in the RAS-MAPK signaling pathway, a central regulator of cell growth, proliferation, and survival. It functions as a molecular switch, cycling between active (GTP-bound) and inactive (GDP-bound) states, dictating when cells should divide. Mutations in KRAS are among the most common oncogenic drivers across human cancers, found in approximately 25-30% of all solid tumors, including high prevalence in pancreatic, colorectal, and lung cancers.
For decades, KRAS was famously dubbed "undruggable." Its smooth, globular surface lacked discernible binding pockets that could be exploited by small molecule drugs, rendering conventional drug discovery efforts largely fruitless. This presented a significant therapeutic void, leaving millions of cancer patients with limited targeted treatment options. The scientific community’s persistent efforts, however, began to yield breakthroughs in the late 2010s, specifically targeting the KRAS G12C mutation. This particular mutation, where a glycine residue at position 12 is replaced by cysteine, not only locks KRAS in its perpetually active, growth-promoting state but, crucially, also creates a small, transient binding groove adjacent to the cysteine residue. This groove became the Achilles’ heel that drug developers had long sought.
The advent of first-generation KRAS G12C inhibitors, such as sotorasib (Lumakras/Lumykras) from Amgen and adagrasib (Krazati) from Mirati Therapeutics (now part of Bristol Myers Squibb), marked a watershed moment. These drugs were designed to covalently attach to the mutant cysteine, trapping KRAS G12C in its inactive state. While these agents demonstrated clinical efficacy and received accelerated approvals for specific indications like non-small cell lung cancer, their impact was often limited by the inherent biology of KRAS. As Jane Healy, Vice President and Head of Oncology Early Development at Merck Research Laboratories, explained, "Because KRAS is such an important protein involved in so many cellular processes, resistance to these medications happens quickly and is quite common, since there are a lot of overlapping pathways that interact with KRAS." This rapid emergence of resistance underscored the need for more robust and sustainable therapeutic strategies. The first-generation inhibitors primarily targeted the fraction of KRAS molecules that transiently cycled into the inactive state, whereas in aggressive cancer cells, the majority of KRAS molecules often remain in the active, oncogenic conformation.
Merck’s Differentiated Approach: Prioritizing Combinability and Potency
Recognizing the limitations of existing KRAS G12C inhibitors, Merck strategically designed calderasib with a dual focus: high specificity for mutant KRAS and, critically, exceptional combinability with other therapeutic agents. This represented a nuanced shift from pursuing maximum standalone potency to achieving superior and more durable responses through synergistic combinations.
"We designed it to be highly specific to mutant KRAS, thereby minimizing interaction with the wild-type version and reducing toxicity, but we also designed it with combinability in mind," Healy reiterated, highlighting the deliberate engineering behind calderasib. This specificity is crucial for reducing off-target effects and improving the drug’s safety profile, making it a more suitable backbone for combination regimens. The rationale is clear: by mitigating toxicity from the individual agent, the therapeutic window for combination therapies can be widened, allowing for the inclusion of other potent drugs that might otherwise be dose-limiting.
This combinability thesis is predicated on overcoming the complex resistance mechanisms that cancer cells rapidly develop against KRAS G12C monotherapies. Cancer’s ability to activate bypass pathways or adapt to single-agent inhibition necessitates a multi-pronged attack. By designing calderasib to integrate seamlessly with other established or emerging cancer therapies, Merck aims to disrupt these escape routes more effectively and achieve deeper, more durable responses. This strategy implicitly acknowledges the intricate signaling networks within cancer cells and the need for comprehensive inhibition rather than isolated targeting.
KANDLELIT-001 Phase 1 Trial: Initial Efficacy and the Combinability Proof-of-Concept
The initial clinical validation for calderasib’s design philosophy emerged from the KANDLELIT-001 Phase 1 trial, a crucial study designed to assess the drug’s safety, pharmacokinetics, and preliminary efficacy in patients with KRAS G12C-mutated solid tumors. The results presented from this trial provided compelling evidence supporting Merck’s combinability thesis.
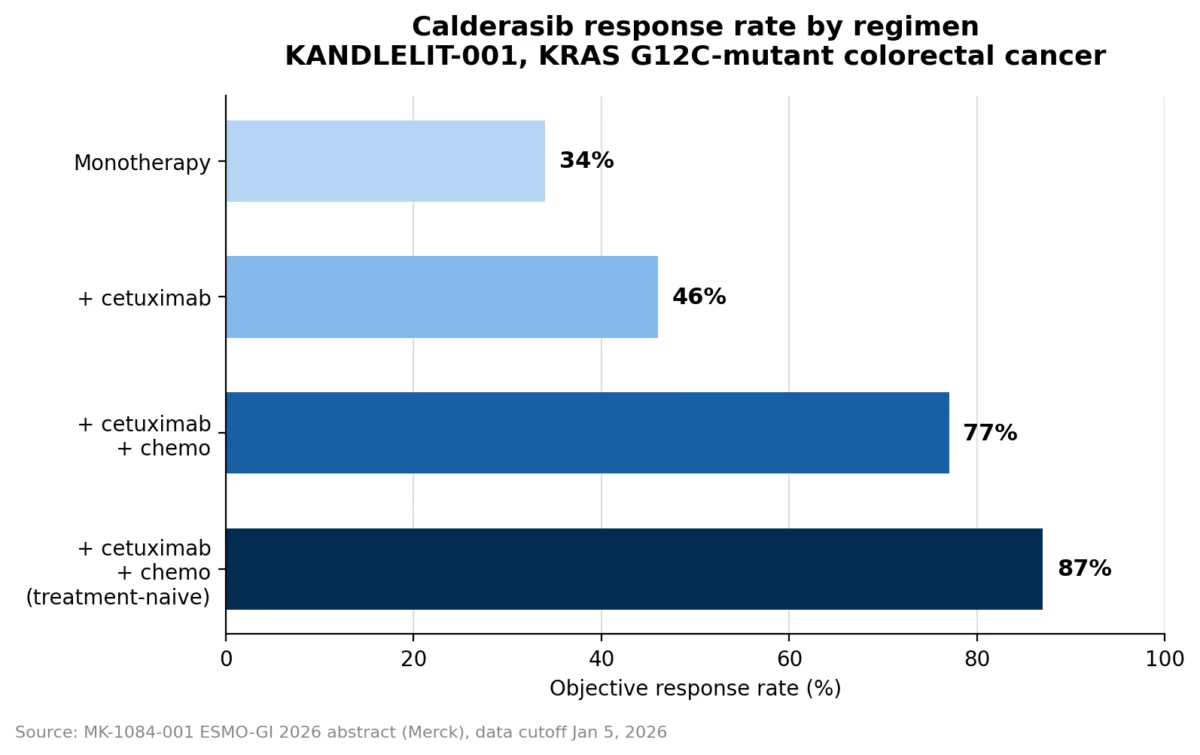
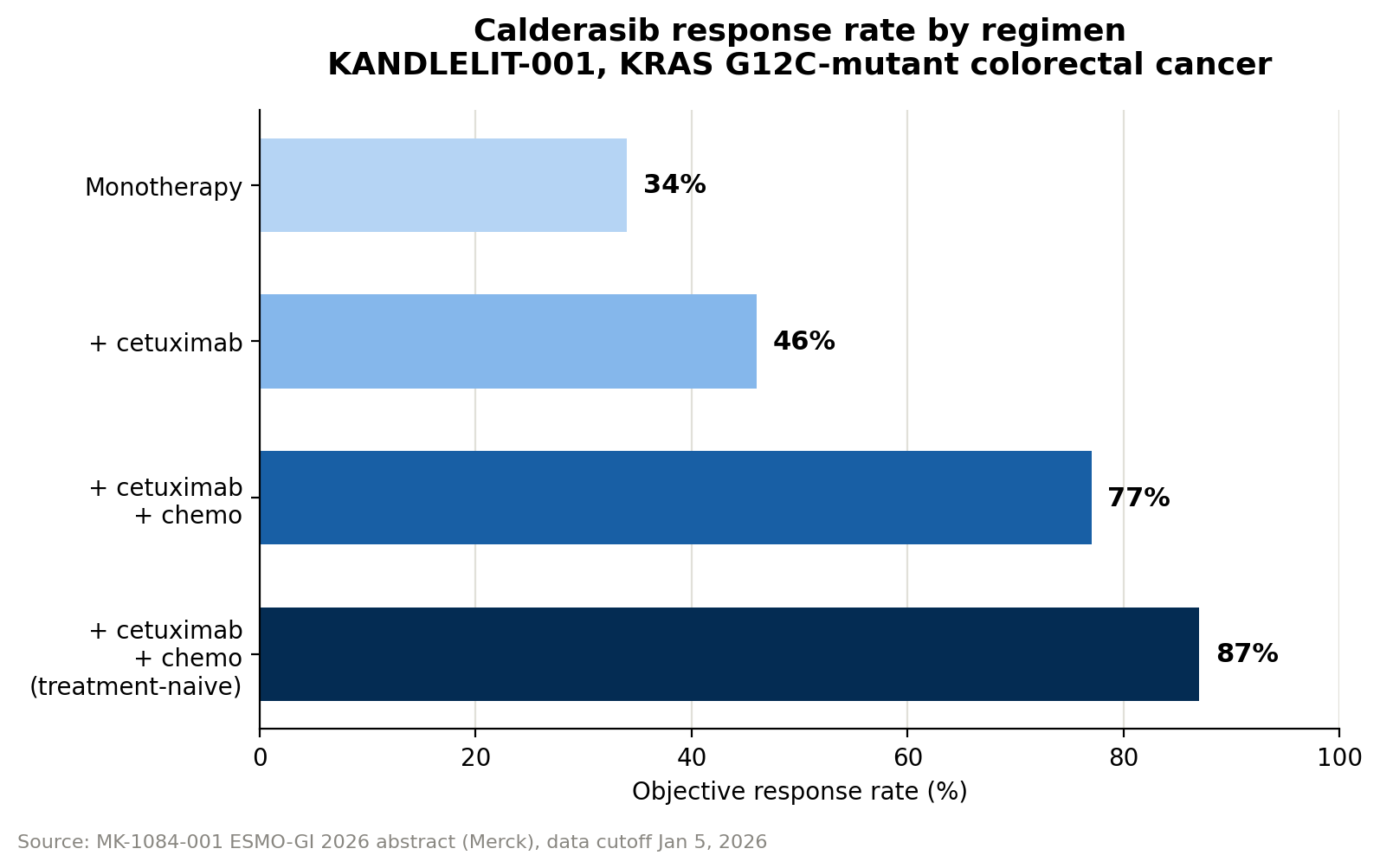
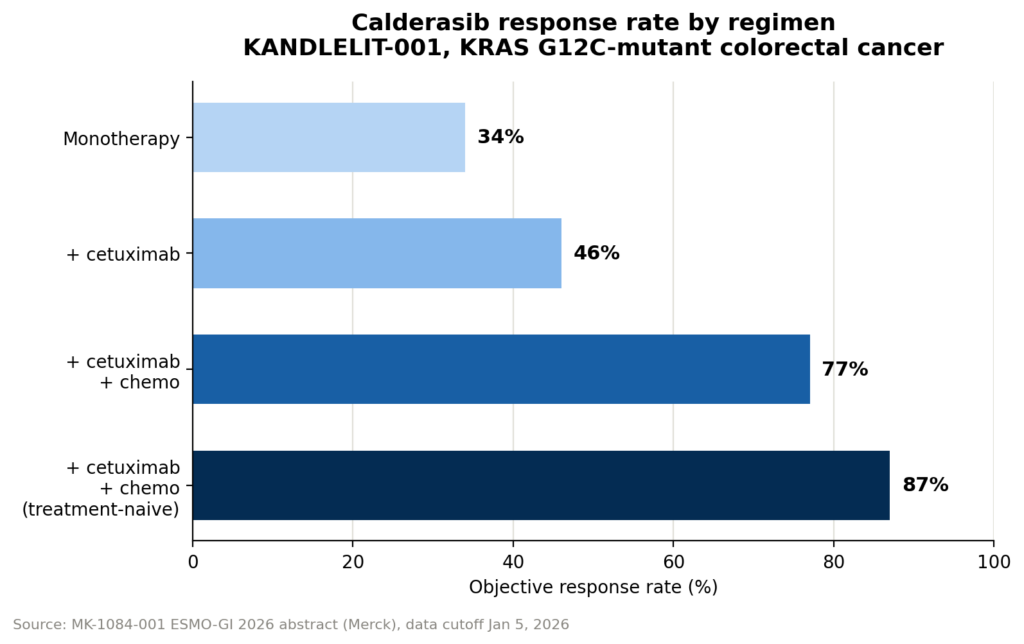
As a monotherapy, calderasib demonstrated an objective response rate (ORR) of 34%. While respectable, the true potential of the drug became evident when combined with other agents. In combination with cetuximab, an epidermal growth factor receptor (EGFR) inhibitor commonly used in colorectal cancer, the ORR significantly increased to 46%. The most striking improvements were observed in a triplet regimen, combining calderasib with cetuximab and chemotherapy (specifically FOLFOX, a standard regimen for colorectal cancer), where the ORR soared to 77%. For patients who had not yet received any prior systemic therapy (first-line setting), the triplet’s response rate climbed even higher, reaching an impressive 87%.
These data strongly suggest that calderasib’s design facilitates potent synergistic interactions, particularly in the context of colorectal cancer where EGFR inhibition and chemotherapy are foundational treatments. The sequential increase in ORR from monotherapy to doublet to triplet regimens provides a powerful illustration of the drug’s intended combinability and its potential to enhance established therapeutic protocols.
From a safety perspective, calderasib as a monotherapy was generally well-tolerated, with only 9% of patients experiencing Grade 3 or 4 drug-related adverse effects (AEs). As expected, the combination regimens led to an increase in AEs, with 20% of patients in the doublet arm and 42% in the triplet arm experiencing Grade 3 or 4 drug-related events. However, Jane Healy maintained that "the combination appears manageable and reflective of the profiles of those individual agents," indicating that the observed toxicities were consistent with the known side-effect profiles of cetuximab and chemotherapy, and did not suggest unexpected synergistic toxicities from calderasib itself. This manageability is critical for combination strategies, as unacceptable toxicity would negate any efficacy gains. It is important to note that this was a relatively small, non-randomized dataset, and larger, randomized controlled trials will be necessary to definitively confirm these efficacy and safety profiles.
The Power of Precision: Tracking Response via Circulating Tumor DNA (ctDNA)
Beyond clinical response rates, Merck also highlighted the utility of an advanced biomarker strategy in monitoring treatment efficacy: tracking the variant allele fraction (VAF) of KRAS G12C in circulating tumor DNA (ctDNA). ctDNA refers to fragments of tumor DNA shed into the bloodstream, which can be collected via a simple blood draw (liquid biopsy). The VAF represents the fraction of these ctDNA fragments carrying the specific G12C mutation.
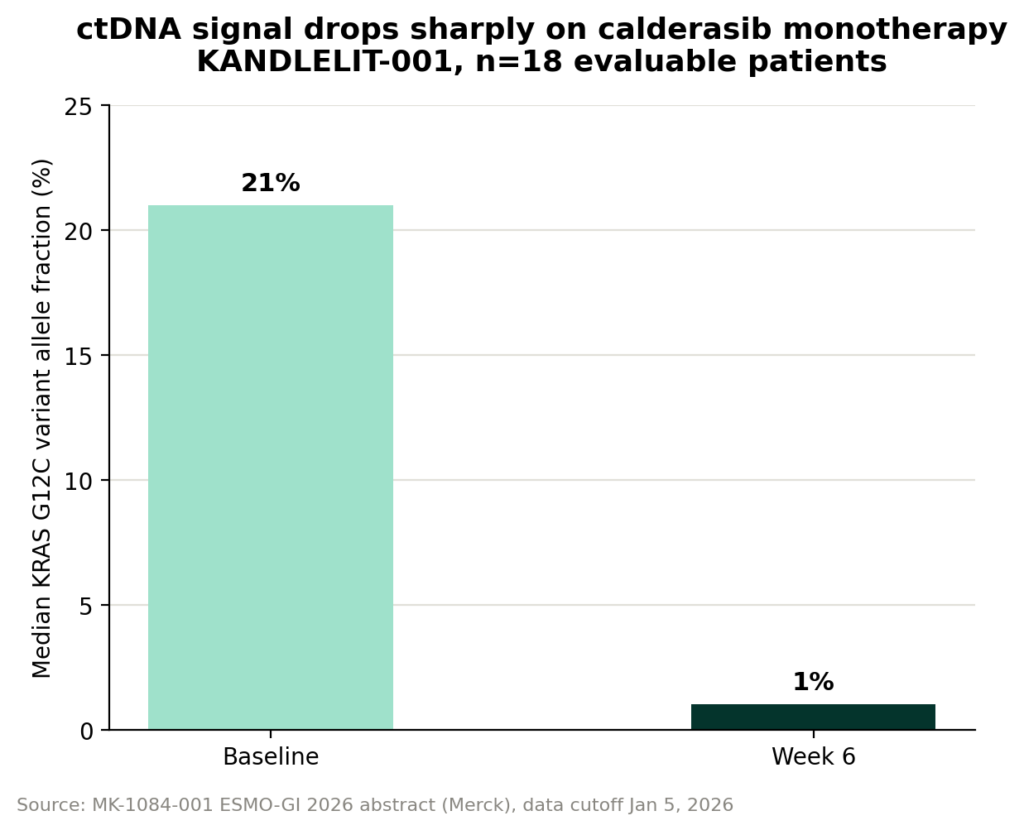
Researchers in the KANDLELIT-001 Phase 1 trial diligently collected ctDNA at various points throughout treatment to measure how calderasib decreased the KRAS G12C VAF. VAF serves as a highly sensitive and dynamic biomarker for tumor burden, providing an indirect measure of the number of mutant tumor cells circulating and shedding DNA. A decline in VAF typically indicates tumor shrinkage or eradication, while a rise can signal tumor growth, sometimes even before it becomes visible on conventional imaging scans.
Healy underscored the significance of this monitoring: "If you track the KRAS G12C variant allele fraction over the course of treatment, it declines, and we can track that across all patients in the study. The reduction in variant allele fraction in the blood correlates quite nicely with the responses we’re seeing by imaging." In the monotherapy arms, calderasib reduced VAF by a median of approximately 95%, dropping from 21% at baseline to 1% at week 6, based on data from 18 ctDNA-evaluable patients. Healy confirmed that this VAF-response correlation extends across the full study population, including the combination arms, with detailed figures expected in future presentations.
Measuring VAF via blood draws offers several distinct advantages over traditional imaging techniques for monitoring tumor burden. It is generally faster, less invasive, cheaper, and less burdensome for patients. This opens the door to more frequent monitoring between scheduled scans, potentially allowing clinicians to detect early signs of resistance or disease progression much sooner than imaging would permit, enabling more timely treatment adjustments. However, it’s also important to acknowledge that VAF is a relative fraction, not an absolute measure of tumor burden, and can be influenced by factors such as the total amount of ctDNA being shed, not just the mutant fraction. Despite this, its predictive and correlative power makes it an invaluable tool in precision oncology.
Merck’s Pioneering Tumor-Agnostic Strategy: A Blueprint for Development
The biomarker-first, tumor-agnostic approach is not a novel concept for Merck; rather, it is a well-established regulatory and development strategy that the company has successfully pioneered. This strategic framework, which prioritizes a specific genetic mutation or biomarker irrespective of the tumor’s anatomical origin, has fundamentally reshaped aspects of oncology drug development and regulatory approvals.
Jane Healy highlighted Merck’s historical leadership in this area: "Merck actually had the first tumor-agnostic approval for a drug, with pembrolizumab, through our KEYNOTE-158 program… That was the first tumor-agnostic biomarker approval for a drug." This landmark approval for pembrolizumab, an immune checkpoint inhibitor, was based on microsatellite instability-high (MSI-High) status, a marker indicating deficient mismatch repair genes. The KEYNOTE-158 trial demonstrated that patients with MSI-High tumors exhibited a consistently higher response rate to pembrolizumab across various tumor types, regardless of their organ of origin. This was further corroborated by retrospective data from other pembrolizumab trials.
Pembrolizumab subsequently gained a second tumor-agnostic approval based on tumor mutational burden (TMB-High), solidifying this innovative regulatory pathway. "So it’s now a precedented approach, and we’re proud to have been first to use that strategy," Healy affirmed. This success with pembrolizumab established a crucial precedent, demonstrating that treatments could be effectively approved and administered based on specific molecular characteristics of the tumor, rather than being confined to traditional organ-specific indications.
Merck is now applying this same proven strategy to calderasib. "We have a study looking at calderasib activity across tumor types — any patient with a KRAS G12C-mutated solid tumor can enroll — taking a biomarker-driven approach rather than a tumor-type-specific one," Healy explained. This pan-tumor study allows patients with a KRAS G12C-mutated solid tumor, irrespective of its original site, to qualify for enrollment. This mirrors the logic of the pembrolizumab trials, focusing on the genetic driver mutation rather than the tissue of origin. This consistent application of the tumor-agnostic strategy, spanning nearly a decade and two different transformative drugs, suggests it is a durable development paradigm for Merck, not merely a one-time regulatory maneuver. The success of this strategy for calderasib, however, will ultimately hinge on the robustness of the accumulating clinical data.
Looking Ahead: Future Trials and the Evolving Landscape of Precision Oncology
The initial findings from KANDLELIT-001 and Merck’s strategic biomarker-driven approach lay the groundwork for the next crucial phase of calderasib’s development. The Phase 3 KANDLELIT-012 trial is already planned, designed to evaluate calderasib in combination with cetuximab and chemotherapy in first-line KRAS G12C-mutant colorectal cancer (CRC). This trial will be a definitive test of the combinability thesis in a specific, high-need patient population, seeking to establish calderasib as a new standard of care.
The implications of calderasib’s development extend beyond just another drug for KRAS G12C. It represents a broader paradigm shift in oncology drug design, emphasizing rational combination strategies from the outset. By designing a drug that is not only highly specific but also highly combinable, Merck is addressing the inherent challenges of rapid resistance and pathway redundancy that plague targeted therapies. This approach acknowledges that complex diseases like cancer often require multi-faceted interventions.
Furthermore, the continued reliance on advanced liquid biopsy techniques, like VAF monitoring, signals a future where cancer treatment is even more personalized and dynamic. The ability to frequently and non-invasively track tumor response and detect early signs of progression or resistance could revolutionize patient management, allowing for timely treatment adjustments and potentially extending progression-free and overall survival.
The competitive landscape for KRAS G12C inhibitors is intensifying, with several companies developing next-generation compounds that aim to improve upon the first wave. Merck’s calderasib, with its distinct emphasis on combinability and a well-established tumor-agnostic development pathway, is strategically positioned to carve out a significant niche. Should the robust results from KANDLELIT-001 be replicated and confirmed in larger, randomized Phase 3 trials, calderasib could offer a powerful new option for patients with KRAS G12C-mutated cancers, particularly those for whom existing therapies have proven inadequate or who rapidly develop resistance. This would represent not just a victory for Merck, but a significant advancement in the ongoing battle against one of cancer’s most challenging molecular targets.