
The dramatic emergence of GLP-1 receptor agonists has undeniably revolutionized the landscape of obesity treatment, driving pharmaceutical giants like Eli Lilly to unprecedented market valuations exceeding $1 trillion. Yet, amidst the fervent optimism and widespread adoption, a nuanced and increasingly critical perspective is taking root within the scientific and medical communities. This perspective, articulated by industry veterans such as Mark Bagnall, CEO of Phenomix Sciences, draws a parallel between the current enthusiasm for GLP-1s and past technological breakthroughs like the internet, which, despite their transformative power, ultimately proved not to be universal panaceas. The growing consensus points towards precision medicine as the inevitable evolution, recognizing that the complexities of obesity demand a tailored approach far beyond any single "silver bullet" solution.
The GLP-1 Phenomenon: A Triumphant Rise with Emerging Caveats
The past few years have witnessed an extraordinary surge in the use of GLP-1 medications for weight loss. By 2025, an estimated 30 million Americans were utilizing these therapies, a testament to their efficacy in achieving significant weight reduction for many individuals. This widespread adoption has fueled an economic boom, catapulting companies like Eli Lilly to the forefront of the pharmaceutical industry, largely on the back of global demand for its obesity and diabetes medications such as Mounjaro (tirzepatide) and Zepbound (tirzepatide). The market narrative has often portrayed GLP-1s as a definitive, one-size-fits-all solution, a perception heavily influenced by extensive marketing campaigns.
However, beneath the surface of this success story, a more cautious narrative is emerging. A survey conducted by Phenomix Sciences revealed that only 33% of patients actually perceive GLP-1s as a definitive solution, suggesting a gap between marketing portrayals and real-world patient experience. This skepticism is not isolated; many scientists and healthcare professionals are increasingly vocal about the dangers of overconfidence in a singular treatment paradigm for a condition as multifactorial as obesity.
Industry Insiders Signal a Shift: Beyond the Monotherapy Model
The pharmaceutical industry itself, often a bellwether for future trends, is already hedging its bets. Mark Bagnall observes that the sheer volume of drugs in development—over 200 new compounds, according to TD Cowen’s 2025 data, covering 68 different mechanisms of action—serves as compelling evidence that drug companies do not view GLP-1s as ultimate panaceas. This robust pipeline includes not only variations of GLP-1s but also an array of entirely novel therapeutic classes, signaling a collective industry understanding that a diverse arsenal of solutions will be required to effectively combat the global obesity crisis.
International health organizations echo this sentiment. The World Health Organization (WHO), in its December 2025 guideline, issued a conditional recommendation for GLP-1 therapies, explicitly framing them as merely one component within a broader, comprehensive approach. The WHO emphasized that medication alone is insufficient, stressing the indispensable role of healthy diets, regular physical activity, and sustained support from health professionals. This official stance underscores a critical shift from a pharmacological-centric view to a holistic patient management strategy, acknowledging the complexity of obesity as a chronic disease requiring multifaceted interventions.
The Overlooked Challenge: Side Effects and Patient Adherence
While GLP-1s offer significant benefits, they are not without drawbacks. The most commonly reported side effects are transient gastrointestinal issues, including nausea, vomiting, diarrhea, and constipation. However, more concerning long-term risks include potential muscle and bone density loss. Alarmingly, the Phenomix survey found that only 45% of patients were fully aware of these risks, with 17% entirely unaware. This lack of awareness can contribute to patient dissatisfaction and, ultimately, discontinuation of treatment.
A significant review published by the American Heart Association in October 2024 further highlighted these concerns, citing studies indicating that less than half of the weight lost with GLP-1 medications typically originates from fat mass, with a substantial proportion attributable to muscle mass. This is a critical clinical consideration, especially for older or already frail patients. As Bagnall points out, "You have to be really thoughtful, because there is a general health benefit to muscle mass – but at some point, if you’re already weak and older, now we go into a whole other category of issues: falls, broken bones." The financial burden on patients is also considerable, with many reporting out-of-pocket expenses of up to an additional $1,000 to manage these side effects, on top of the already high cost of the medications themselves, which are often not fully covered by insurance.
For some individuals, these side effects are not merely transient but can be permanent and debilitating, forcing them to discontinue treatment. The psychological impact of such an experience can be profound. "They’ve been told there’s a silver bullet. And then six months later, nothing happened," Bagnall explains. "I think where you really feel despair as a patient is when the thing that has been promised to you as the answer to your problems fails." This underscores the urgent need for a more personalized approach that can predict and mitigate such adverse outcomes.
Precision Medicine: The Path Forward in Obesity Management
The variability in patient response to GLP-1s, particularly concerning side effects, strongly suggests underlying genetic differences. This is where precision medicine offers a compelling solution. Phenomix Sciences is at the forefront of this movement, developing genetic tests designed to identify patients who are most likely to benefit from GLP-1s and, critically, those who may be intolerant to the medications, experiencing severe or permanent side effects. This proactive approach aims to prevent patient suffering and improve treatment efficacy by matching the right patient with the right therapy from the outset.
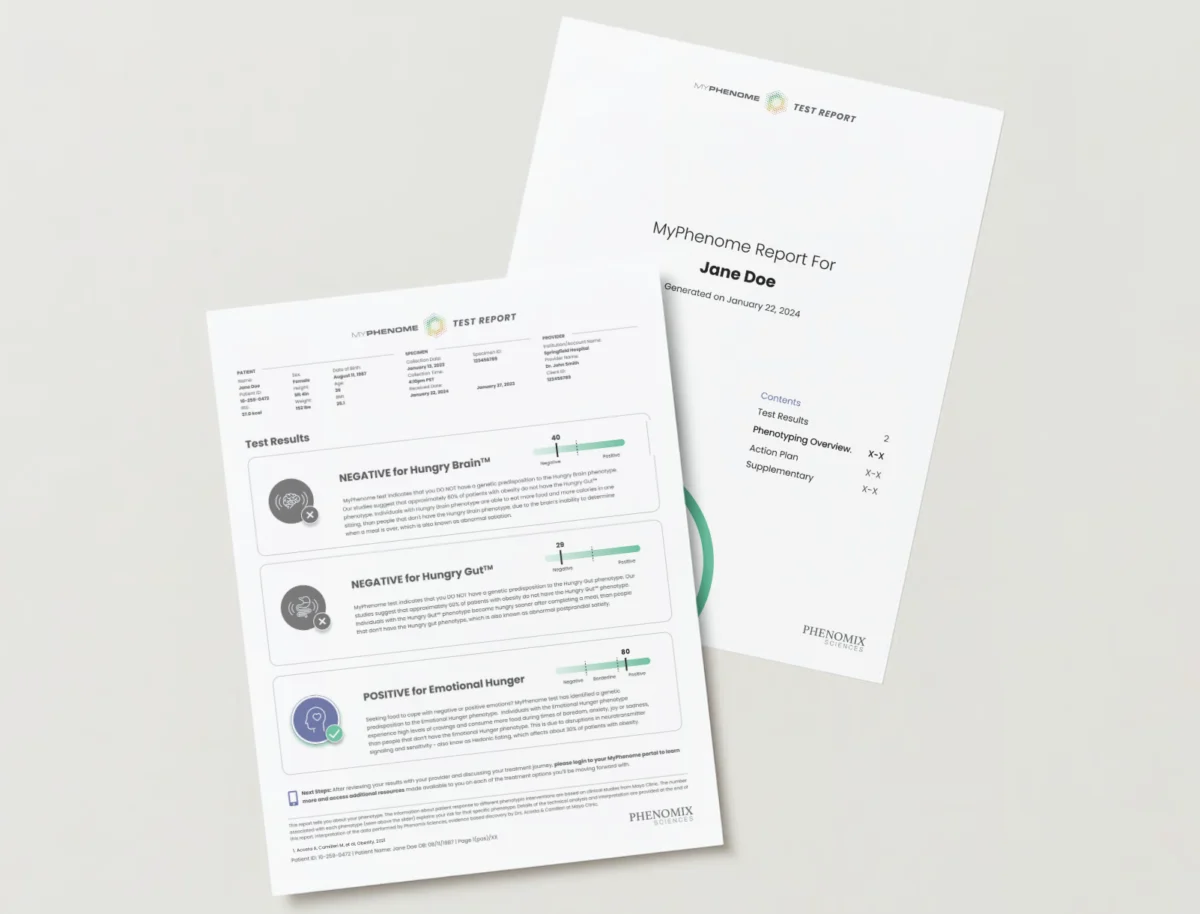
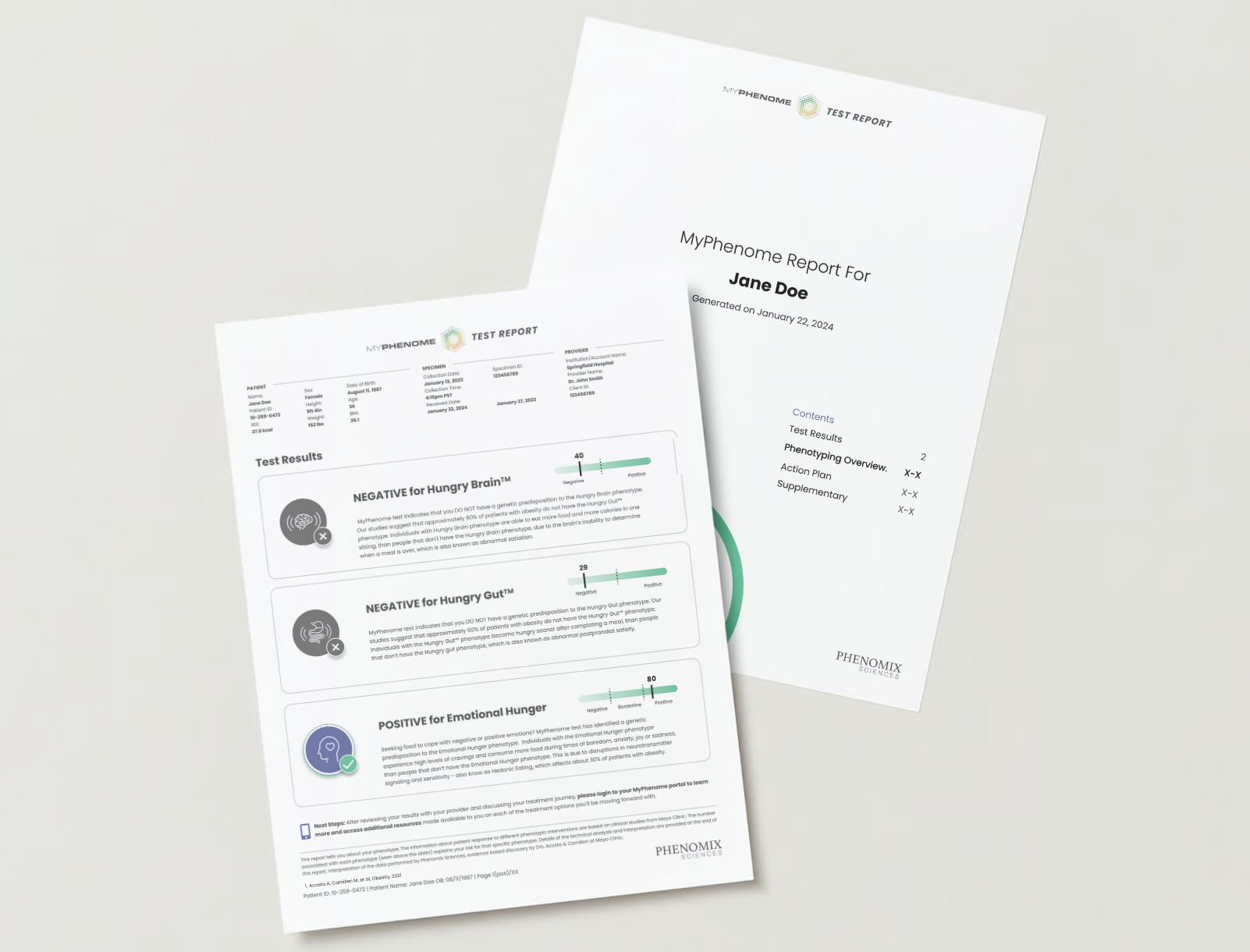
The philosophical foundation of Phenomix’s work is rooted in groundbreaking Mayo Clinic research that identified four distinct obesity subtypes, or "phenotypes": "hungry brain," "hungry gut," "emotional hunger," and "slow burn." These phenotypes are delineated by differences in the gut-brain axis, specifically how the gut communicates hunger and fullness signals to the brain, influencing satiety and metabolic rate.
This phenotypic classification provides a robust framework for personalized treatment. For instance, patients exhibiting the "hungry brain" phenotype, characterized by dysregulated satiety signals originating from the central nervous system, tend to respond favorably to medications like phentermine or extended-release topiramate. Conversely, individuals with "emotional hunger," where psychological factors drive eating behaviors, often show better outcomes with combination therapies such as Contrave (bupropion/naltrexone). The "hungry gut" phenotype, marked by rapid gastric emptying and insufficient satiety signaling from the gut, is precisely where GLP-1 receptor agonists demonstrate their greatest efficacy. The "slow burn" phenotype, characterized by a lower resting metabolic rate, may require interventions targeting energy expenditure.
This precision approach can significantly enhance the effectiveness of existing medications. For example, older drugs like Qsymia (phentermine/topiramate extended-release), while demonstrating an average weight loss of around 10% in general populations, can achieve a remarkable 17% weight loss in "hungry brain" patients—a figure comparable to the best outcomes seen with GLP-1s. This highlights the potential to optimize the use of a broader range of pharmaceutical agents by accurately identifying the most responsive patient populations. Bagnall emphasizes the profound role of genetics, stating that it can explain 70% to 80% of a patient’s response to obesity drugs.
Phenomix’s Innovations and a Vision for the Future

Phenomix is actively developing tests, such as their MyPhenome test, not only to categorize patients by phenotype but also to specifically identify "super intolerant" individuals who are prone to severe, permanent nausea or vomiting when treated with GLP-1s. Such a test could fundamentally transform the prescribing process, ensuring that patients avoid initiating a medication that will cause them significant and lasting distress. This represents a critical step towards realizing the promise of precision medicine in obesity.
Bagnall envisions a future where obesity treatment mirrors the sophisticated, individualized approach currently employed in oncology. "It’ll be like oncology, but on a mass scale," he predicts. Just as cancer patients undergo genetic profiling to determine the most effective chemotherapy or targeted therapy, individuals with obesity will receive personalized diagnostics to guide their treatment plan.
Looking ahead, Bagnall forecasts a market brimming with therapeutic options. He anticipates that within the next decade, there could be as many as 50 different obesity drugs available. This proliferation of specialized medications, combined with advanced diagnostic tools, will enable a truly nuanced and effective approach to managing obesity. His long-term vision is even more ambitious: in 20 years, he believes, "we will have cured it." This statement, while bold, reflects the transformative potential of moving beyond a simplistic, one-size-fits-all mentality towards a deeply individualized and scientifically grounded strategy for tackling one of the most pervasive global health crises.
Broader Implications for Healthcare and the Market
The shift towards precision medicine in obesity carries profound implications across the healthcare ecosystem. For pharmaceutical research and development, it signifies a move away from blockbuster drugs targeting broad populations towards a diversified portfolio of specialized therapies. This will necessitate greater investment in diagnostic tools and companion diagnostics, similar to trends seen in oncology.
For healthcare providers, it means a more complex but ultimately more rewarding approach to patient care. Clinicians will need to be equipped with the knowledge and tools to accurately phenotype patients and interpret genetic test results, enabling them to make truly informed treatment decisions. This will likely involve enhanced training and the integration of specialized obesity clinics capable of offering comprehensive, multidisciplinary care.
Economically, while the upfront costs of genetic testing and personalized diagnostics may seem higher, the long-term benefits could be substantial. By reducing trial-and-error prescribing, minimizing adverse events, improving patient adherence, and optimizing treatment efficacy, precision medicine has the potential to lower overall healthcare expenditures associated with obesity and its comorbidities. Furthermore, more effective treatments mean healthier populations, leading to increased productivity and reduced societal burden.
Ultimately, the journey beyond the "silver bullet" of GLP-1s is not a rejection of their efficacy but an evolution towards a more sophisticated understanding of obesity itself. By embracing precision medicine, the medical community is poised to usher in an era where personalized care, guided by genetic insights and phenotypic understanding, offers genuine hope for effectively managing and, perhaps one day, curing this complex disease. The $1 trillion obesity market, therefore, is not just a measure of current success but a massive canvas for future innovation driven by scientific precision.











Leave a Reply