The annual scientific sessions of the American Diabetes Association (ADA) this week served as a dual-faceted arena, showcasing both groundbreaking advancements in metabolic disease therapeutics and an unexpected, highly public demonstration of scientific advocacy that led to the removal of several prominent researchers. Pharmaceutical giants Eli Lilly, Novo Nordisk, AstraZeneca, and Pfizer unveiled a trove of new clinical and preclinical data for their next-generation GLP-1 receptor agonists and related compounds, signaling a rapid evolution in the treatment of type 2 diabetes and obesity. Simultaneously, the conference was marked by a dramatic incident where a group of experts was escorted out by police for distributing an editorial critical of the Trump administration’s science policies, raising questions about academic freedom and appropriate forms of protest within scientific gatherings.
A Conference Interrupted: The Unfolding Controversy Over Scientific Freedom
The ADA conference, a cornerstone event in the global diabetes community, is typically a forum for collegial exchange and the presentation of scientific breakthroughs. However, this year, a political undercurrent erupted into public view. The catalyst was an editorial titled "Misguided Brushes of a Pen Continue to Dismantle" published in Diabetes Care, the ADA’s flagship journal. This editorial sharply criticized the science policies of the Trump administration, detailing the adverse effects of federal funding cuts, restrictions on scientific communication, and other actions that, in the authors’ view, significantly hampered diabetes research and public health initiatives. The piece underscored concerns about the politicization of science and its potential long-term consequences for a field reliant on robust, unfettered investigation.
The incident unfolded shortly before a scheduled address by Jay Bhattacharya, director of the National Institutes of Health (NIH), a key federal agency whose policies and funding directly impact the research landscape. A group of prominent researchers began distributing copies of the critical editorial near the conference venue. This act of protest was intended to draw attention to the perceived erosion of scientific integrity and independence under the administration’s policies, particularly from those responsible for shaping the national research agenda.
According to firsthand accounts, security staff promptly intervened. Aaron Kelly, a professor of pediatrics at the University of Minnesota and one of the researchers involved, reported to The New York Times that security personnel asked them to step outside and attempted to confiscate the distributed papers. The researchers, however, sought to re-enter the convention through a different entrance, determined to continue their message. Their attempt was met by an escalated response: event security, now accompanied by police officers, informed them that any further attempt to enter the premises would be considered trespassing and would result in arrest.
In the aftermath, five of the researchers involved were officially barred from participating further in the conference. This decision carried significant implications, as some of those excluded were scheduled to present their own research findings, effectively silencing their scientific contributions in addition to their political protest. The incident sparked a lively debate within the scientific community and beyond, pitting the conference organizers’ need to maintain order and a politically neutral environment against the researchers’ assertion of their right to express concerns critical to the scientific enterprise. While the ADA did not issue a detailed public statement specifically on the removal of the researchers, such actions by conference organizers are typically justified under codes of conduct designed to ensure a professional and respectful environment, though the application of such rules in cases of political expression remains a contentious issue. The episode underscored the growing tension between scientific independence and the political realities that increasingly influence research funding and policy.
GLP-1 Innovations: A New Horizon in Metabolic Disease Treatment
Despite the political drama, the scientific presentations at ADA were nothing short of transformative, particularly in the realm of GLP-1 (glucagon-like peptide-1) receptor agonists and their analogues. These drugs have already revolutionized the treatment of type 2 diabetes and obesity, and the data presented this week suggested that an even more potent and versatile generation is on the horizon. The focus was on enhanced weight loss, improved glycemic control, and the potential to address a broader spectrum of obesity-related comorbidities.
Eli Lilly’s Retatrutide: A Triple Agonist Poised for Broad Impact
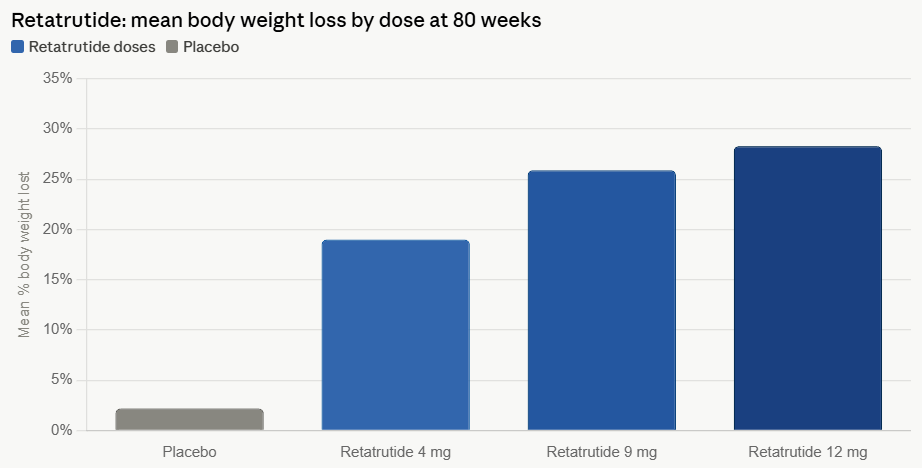
Eli Lilly presented compelling Phase 3 results for its investigational triple agonist, retatrutide, which targets GLP-1, GIP (glucose-dependent insulinotropic polypeptide), and glucagon receptors. This multi-receptor approach is designed to harness synergistic pathways for enhanced metabolic effects, building on the success of dual agonists like tirzepatide (Mounjaro/Zepbound).
The trial data revealed extraordinary efficacy in weight management, with participants achieving an average body weight loss of 28.3% over 80 weeks on the highest dose. This figure significantly surpasses the weight loss observed with current market leaders, including tirzepatide, which typically demonstrates around 20-22% weight reduction in similar timeframes. Such a profound impact on body weight positions retatrutide as a potential game-changer in the fight against severe obesity.
Beyond weight loss, retatrutide showcased remarkable benefits for obesity-related comorbidities. The drug reduced knee osteoarthritis pain by up to 73.1% and improved the severity of moderate-to-severe obstructive sleep apnea by 60.6%. Both conditions are strongly linked to obesity, and the ability of a single therapeutic agent to ameliorate these debilitating complications highlights retatrutide’s potential to significantly improve patients’ overall health and quality of life. Ania Jastreboff, the lead investigator, emphasized this point, stating, "These findings demonstrate what may be possible when we treat obesity and impact overall health, and what this could mean for people living with obesity and its related complications."
For patients with type 2 diabetes, retatrutide delivered substantial improvements in glycemic control, reducing HbA1c by up to 2%. A remarkable 90% of participants achieved an HbA1c below 7%, aligning with the ADA’s general target for type 2 diabetes management. The drug also demonstrated positive effects on cardiovascular risk factors, reducing triglycerides by up to 41%, non-HDL cholesterol by 24.2%, and systolic blood pressure by 12.3 mmHg. These comprehensive metabolic improvements underscore retatrutide’s potential as a holistic treatment for individuals grappling with the multifaceted challenges of diabetes and obesity.
In terms of tolerability, Lilly reported that retatrutide’s safety profile was generally consistent with other GLP-1 class medications. The most common adverse effects included gastrointestinal issues such as nausea, diarrhea, constipation, and vomiting, which are typical for this class of drugs. Approximately 14.2% of participants on the highest dose experienced upper respiratory tract infections. A limited incidence of dysesthesia, a condition characterized by abnormal or unpleasant sensations, was also observed, a side effect that has been noted to a minor extent with related drugs. These findings suggest that while side effects are present, they are largely manageable and align with expectations for such potent metabolic therapies.
Novo Nordisk’s CagriSema: Amylin-GLP-1 Synergy and Market Positioning

Novo Nordisk presented new Phase 3 data for CagriSema, a novel combination therapy that pairs an amylin analog with a GLP-1 receptor agonist. The REIMAGINE program, comprising multiple Phase 3 trials, demonstrated significant reductions in HbA1c and body weight compared to its comparators. This dual-action mechanism aims to leverage the synergistic effects of both hormones, which play crucial roles in glucose homeostasis and appetite regulation.
Martin Holst Lange, executive vice president, chief scientific officer, and head of Research and Development at Novo Nordisk, highlighted the drug’s potential: "With these findings, CagriSema has the potential to be the first amylin and GLP-1 combination therapy that addresses blood glucose control with reductions in bodyweight for people living with type 2 diabetes."
A key comparative finding was CagriSema’s performance against semaglutide (Ozempic/Wegovy), Novo Nordisk’s own market-leading GLP-1. CagriSema achieved a greater reduction in both HbA1c and body weight. Specifically, the highest dose of CagriSema led to a 14.2% reduction in body weight over 68 weeks, outperforming the 10.2% reduction observed with the same dose of semaglutide. This suggests a clear advantage over monotherapy with semaglutide, potentially offering a more potent option for patients requiring greater weight loss and glycemic control.
However, earlier this year, another Phase 3 trial revealed that CagriSema was inferior to Eli Lilly’s tirzepatide (Zepbound), a dual GLP-1/GIP agonist. In that head-to-head comparison, CagriSema achieved 23% weight loss after 84 weeks of treatment, while tirzepatide demonstrated 25.5% weight loss. Addressing this, Martin Lange explained during an investor call that Zepbound "performed unusually well on efficacy compared to what has typically been reported in most previous trials of a similar nature." He pointed out that in a separate Phase 3 trial, tirzepatide in adults with pre-diabetes and obesity achieved an average weight reduction of 22.9% on its highest dose, slightly less than the 25.5% seen in the CagriSema comparator trial, indicating potential variability in trial outcomes. These nuanced comparisons highlight the intense competition and the challenge of establishing clear "best-in-class" status in a rapidly evolving therapeutic landscape.
The Advance of Oral GLP-1s: Convenience and Expanding Options
The pursuit of oral formulations for GLP-1 receptor agonists continues to be a significant area of research, driven by the desire for improved patient convenience and adherence compared to injectable therapies. While oral versions have historically demonstrated less potent weight loss compared to their injectable counterparts, ongoing development aims to bridge this gap while offering a compelling alternative.
AstraZeneca presented promising results for its oral GLP-1, elecoglipron. In clinical trials, elecoglipron achieved an 11.8% weight reduction at 36 weeks and lowered HbA1c by 1.9% at 26 weeks, with 90% of patients reaching an HbA1c below 7%. These results are robust for an oral agent and signal its potential to become a valuable treatment option. Crucially, the drug is now advancing to Phase 3 trials in both obesity and type 2 diabetes, where it will be further evaluated for cardiovascular and kidney outcomes. Demonstrating benefits in these critical areas is increasingly important for regulatory approval and market differentiation.
Ascletis also contributed to the oral GLP-1 narrative with data for its ASC30. In Phase 2 trials, ASC30 showed weight loss of up to 7.7% at week 13. A notable advantage reported was its tolerability profile, with approximately half the rate of vomiting observed compared to orforglipron, another oral GLP-1 in development. Additionally, Ascletis showcased preclinical findings for its oral amylin receptor agonist, ASC37/ASC39, demonstrating selectivity for the human amylin type 1 receptor comparable to eloralintide. These findings suggest the potential for future combination therapies involving oral GLP-1s and amylin agonists, further diversifying treatment strategies.
Pfizer’s Berobenatide: The Promise of Once-Monthly Dosing
Pfizer unveiled data for berobenatide, a novel GLP-1 receptor agonist designed for once-monthly administration. This extended dosing interval represents a significant leap in convenience, potentially enhancing patient adherence and overall treatment experience, which is a key differentiator in a crowded market.
Phase 2b results for berobenatide were impressive, showing a 15.9% weight loss at 32 weeks and a 2.2% reduction in HbA1c at 18 weeks. These efficacy numbers, combined with the convenience of monthly dosing, position berobenatide as a strong contender. Jim List, chief internal medicine officer at Pfizer, articulated the company’s vision: "These data highlight the potential for berobenatide to be the first approved monthly GLP-1 RA peptide and support our extensive Phase 3 program that includes 10 studies for chronic weight management and obesity-related comorbidities."
Pfizer’s commitment to berobenatide is evident in its robust clinical development plan. The VESPER-6 Phase 3 study, which investigates monthly maintenance dosing for berobenatide in adults with obesity or overweight, is actively enrolling participants. Furthermore, the SOLIS-1 Phase 2b study is exploring weekly and monthly maintenance dosing of an ultra-long-acting amylin analog (PF-3945) both as a monotherapy and in combination with berobenatide, signaling Pfizer’s strategic interest in combination therapies to maximize efficacy.
Broader Implications and Future Outlook
The ADA conference 2026 underscored a pivotal moment in metabolic health. The rapid proliferation of GLP-1-based therapies, including triple agonists, amylin combinations, oral formulations, and extended-release injectables, is set to dramatically expand therapeutic options for millions of patients with type 2 diabetes and obesity. This intense competition among pharmaceutical giants is driving innovation, leading to drugs with unprecedented efficacy in weight loss and broader benefits for related comorbidities like cardiovascular disease, sleep apnea, and osteoarthritis. The future of treatment is moving towards more personalized approaches, allowing clinicians to tailor therapies based on individual patient needs, preferences for administration (oral vs. injectable, weekly vs. monthly), and specific comorbidity profiles.
However, the unprecedented protest and subsequent removal of researchers also served as a stark reminder of the broader context in which scientific progress occurs. It highlighted the ongoing tension between scientific independence, the ethical obligations of researchers to advocate for sound science policy, and the organizational demands of large professional conferences. This incident will likely spark further discussions within scientific societies about how to balance open discourse, dissent, and decorum, especially when political issues directly intersect with public health and research funding.
As these investigational drugs move closer to regulatory approval, the focus will shift to real-world effectiveness, long-term safety, access, and affordability. The ADA conference provided a comprehensive snapshot of a field in rapid transformation, promising a future where diabetes and obesity management is more effective, holistic, and tailored than ever before, even as it navigates the complex interplay of science and society.