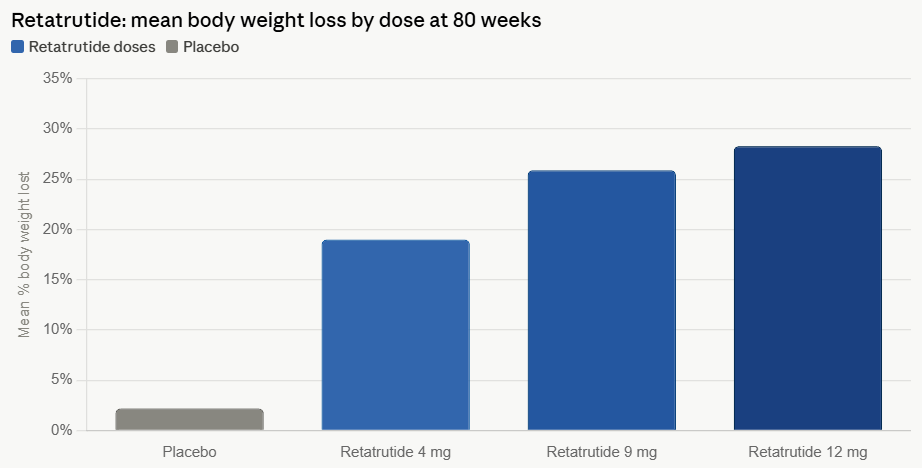
Eli Lilly’s experimental triple hormone receptor agonist, retatrutide, has recently captured significant attention within the medical and pharmaceutical communities following the release of its Phase 3 trial results. The drug, which targets the GLP-1, GIP, and glucagon receptors, has shown an extraordinary average weight loss of 28.3% over 80 weeks when administered at its highest dose. This figure positions retatrutide as potentially the most potent pharmacological agent for obesity treatment to date, surpassing the efficacy observed with other established GLP-1 receptor agonists. However, this remarkable efficacy is accompanied by an increased severity of side effects, including common gastrointestinal issues like nausea and vomiting, along with more distinct concerns such as dysesthesia (abnormal skin sensations) and a notable loss of muscle mass, prompting a nuanced discussion about its overall clinical utility and patient suitability.
The Global Burden of Obesity and the Pharmaceutical Response
Obesity has escalated into a global health crisis, affecting hundreds of millions worldwide and contributing significantly to the prevalence of numerous chronic conditions, including type 2 diabetes, cardiovascular diseases, certain cancers, and musculoskeletal disorders. The World Health Organization (WHO) estimates that globally, over 1 billion people are obese, a number that has tripled since 1975. This epidemic places immense strain on healthcare systems and significantly diminishes the quality of life for affected individuals. For decades, treatment options for obesity were limited, primarily consisting of lifestyle interventions (diet and exercise) and bariatric surgery for severe cases. While highly effective, bariatric surgery is invasive, carries its own risks, and is not suitable or accessible for all patients. This therapeutic gap spurred intensive research into pharmacological solutions that could offer substantial weight loss without surgical intervention.
The landscape of obesity treatment began to transform with the advent of glucagon-like peptide-1 (GLP-1) receptor agonists. Drugs like liraglutide (Saxenda) and semaglutide (Wegovy, Ozempic) marked a paradigm shift, demonstrating clinically meaningful weight reduction by mimicking natural gut hormones that regulate appetite and glucose metabolism. These agents work by slowing gastric emptying, increasing satiety, and reducing food intake. Eli Lilly further advanced this field with tirzepatide (Zepbound, Mounjaro), a dual GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptor agonist. Tirzepatide’s dual action led to even greater weight loss, achieving an average reduction of approximately 20-22% in clinical trials, establishing a new benchmark for pharmacological obesity management. Retatrutide, as a triple agonist, represents the next frontier, aiming to leverage the synergistic effects of three distinct incretin pathways to achieve unprecedented efficacy.
Unpacking Retatrutide’s Mechanism: A Triple Agonist Approach
Retatrutide’s mechanism of action is more complex and potentially more powerful than its predecessors, targeting three key hormone receptors:
- GLP-1 (Glucagon-like peptide-1): This hormone plays a crucial role in glucose homeostasis by stimulating glucose-dependent insulin secretion, suppressing glucagon secretion, slowing gastric emptying, and promoting satiety in the brain, thereby reducing food intake.
- GIP (Glucose-dependent insulinotropic polypeptide): Like GLP-1, GIP enhances insulin secretion in a glucose-dependent manner. Emerging evidence also suggests GIP has broader metabolic roles, including effects on adipose tissue, lipid metabolism, and potentially bone health, making its agonism a valuable component for comprehensive metabolic improvement.
- Glucagon: Traditionally known for its role in raising blood glucose levels by stimulating hepatic glucose production. However, in the context of a multi-receptor agonist, glucagon receptor agonism is hypothesized to contribute to increased energy expenditure and direct satiety signals, potentially through central nervous system pathways. This unique combination is believed to amplify the metabolic benefits, leading to more profound weight loss by simultaneously enhancing satiety, reducing caloric intake, and potentially increasing energy expenditure. This multi-pronged approach distinguishes retatrutide from current single or dual agonist therapies.
TRIUMPH-1: A Deep Dive into Phase 3 Efficacy
The impressive weight loss statistics for retatrutide stem from the TRIUMPH-1 Phase 3 trial, a pivotal study designed to evaluate the efficacy and safety of the triple agonist in adults with obesity or overweight with weight-related comorbidities, excluding individuals with type 2 diabetes. The trial spanned 80 weeks, allowing for a comprehensive assessment of long-term weight management and providing robust data on sustained weight reduction. Participants receiving the highest dose (12 mg) of retatrutide achieved an average body weight reduction of 28.3%. This remarkable figure not only sets a new standard for pharmacological obesity treatments but also brings the efficacy of a pharmaceutical agent into direct comparison with outcomes typically observed with bariatric surgical procedures, which often result in 25-35% excess weight loss over a similar timeframe.
Kenneth Custer, executive vice president and president of Lilly Cardiometabolic Health, underscored the significance of these results, stating, "TRIUMPH-1 highlights the importance of options and the potential for retatrutide to help people across various stages of their obesity journey." He further elaborated on the dose-dependent efficacy, noting that even the 4 mg dose achieved nearly 20% weight loss with one escalation step, while the 12 mg dose delivered a level "long associated with bariatric surgery." Custer emphasized that retatrutide could offer a "patient-centric approach to obesity," complementing Lilly’s existing portfolio, including Zepbound (tirzepatide) and Foundayo, thereby expanding the range of treatment options available to patients based on their individual needs and preferences. This strategic diversification aims to cater to a broader spectrum of patient requirements and therapeutic goals within the obesity management landscape.
The Double-Edged Sword: Increased Side Effects and Tolerability Concerns
While the efficacy data for retatrutide are undeniably groundbreaking, the reported increase in the severity of side effects presents a critical consideration for its real-world application. Common adverse events, consistent with other incretin-based therapies, include nausea and vomiting, often dose-dependent and most pronounced during dose escalation. However, retatrutide’s profile also features distinct concerns like dysesthesia and a significant loss of muscle mass, which could influence patient adherence, quality of life, and long-term health outcomes.
The discontinuation rate due to adverse events serves as a key indicator of a drug’s tolerability and its potential for long-term use. In the retatrutide Phase 3 trials, 11.3% of participants on the highest dose discontinued treatment because of side effects. This figure is notably higher than those reported for other leading GLP-1 agonists: tirzepatide had a discontinuation rate of 6.1%, semaglutide 8.0%, and orforglipron (Lilly’s oral non-peptide GLP-1) 10.3%. This higher rate suggests that while retatrutide offers superior weight loss, a subset of patients may find the side effects too challenging to endure, potentially limiting its broad applicability and necessitating careful patient counseling and management strategies.
Dysesthesia: A Peculiar Adverse Event
One of the more distinctive side effects reported with retatrutide is dysesthesia, experienced by approximately 12.5% of participants on the highest dose. Dysesthesia refers to abnormal, unpleasant sensations such as burning, tingling, or "pins and needles" on the skin, often without an apparent external stimulus. While these events were generally described as mild to moderate and most resolved during treatment, their prevalence is noteworthy. For comparison, orforglipron reported dysesthesia in only 1.2% of participants at its highest dose, while high doses of semaglutide (7.2 mg in experimental trials, a dose higher than currently approved for weight management) caused the side effect in a higher proportion, 22.9% of participants. Other commonly used GLP-1s, such as liraglutide or standard-dose semaglutide (2.4mg Wegovy), have not prominently listed dysesthesia as a significant adverse effect in their product information, making its incidence with retatrutide a point of particular interest.
The exact mechanism underlying dysesthesia in the context of incretin mimetics is not fully understood, but researchers hypothesize several possibilities. One theory points to the activation of glucagon or GLP-1 receptors, which are expressed on central and peripheral nerves. Alterations in nerve signaling pathways due to the drug’s action could manifest as these sensory disturbances. Another proposed cause relates to the metabolic shifts accompanying rapid weight loss and reduced food intake. Transient changes in B vitamins and electrolytes, crucial for optimal nerve health and function, could potentially trigger these sensations. Further research is needed to elucidate the precise etiology and to identify potential mitigation strategies for this specific side effect, which, while often mild, could impact patient comfort and adherence.
The Critical Concern of Lean Mass Loss
While weight loss is the primary goal of these therapies, the composition of that weight loss is increasingly scrutinized. Studies have shown that GLP-1 induced weight loss can comprise a significant proportion of lean tissue, ranging from 20% to 35% of the total weight lost, rather than exclusively fat. This is a critical concern because lean mass, primarily muscle, is essential for metabolic health, strength, mobility, and overall quality of life. The loss of muscle mass can lead to decreased basal metabolic rate, making weight maintenance more challenging, and can contribute to sarcopenia and frailty, particularly in older adults or those with pre-existing muscle weakness.
For orforglipron, trials indicated that an average of 26.9% of the total weight loss was attributable to a loss in lean mass. Similarly, Novo Nordisk’s CagriSema, a dual amylin/GLP-1 agonist, which achieved an average weight loss of 22.7% after 68 weeks in Phase 3 trials, showed a 14.4% reduction in lean soft-tissue mass. Given retatrutide’s unprecedented average weight loss of 70.3 lbs in its trials, applying the 20-35% lean tissue loss range would suggest a potential muscle mass reduction of approximately 14 to 24.6 lbs. This is a substantial amount and raises significant clinical questions regarding long-term functional outcomes. Direct body composition data for retatrutide has not yet been published, but additional results from the Phase 3 trial, which are