Merck’s investigational KRAS G12C inhibitor, calderasib, is making headlines not for its standalone potency but for a strategically different attribute: its designed combinability with other therapeutic agents. This approach marks a significant evolution in the pursuit of effective treatments for cancers driven by the notoriously challenging KRAS G12C mutation, a target once deemed "undruggable." The drug’s development underscores a shift in oncology toward sophisticated combination regimens aimed at overcoming rapid resistance mechanisms and achieving more durable patient responses.
The Enduring Challenge of KRAS-Driven Cancers
The KRAS gene plays a critical role in cellular growth, acting as a molecular switch that cycles between active and inactive states to signal cell division. Mutations in KRAS are among the most prevalent oncogenic drivers across a spectrum of human cancers, including lung, colorectal, and pancreatic cancers. For decades, the smooth, featureless surface of the KRAS protein made it an elusive target for therapeutic intervention, earning it the moniker "undruggable."
The discovery of the G12C mutation offered a glimmer of hope. This specific mutation locks the KRAS protein in its active, cell-growth-promoting state but, crucially, also creates a small, druggable pocket. This structural alteration allowed for the development of covalent inhibitors that could bind to and inactivate the mutant protein. The first generation of these inhibitors, exemplified by sotorasib and adagrasib, demonstrated clinical proof-of-concept by trapping KRAS G12C in its inactive state. However, their efficacy was often limited by the dynamic nature of KRAS, as they primarily targeted the fraction of KRAS molecules that transiently cycled into the inactive conformation. In aggressive cancer cells, the vast majority of KRAS molecules tend to remain perpetually active, leading to inherent resistance challenges.
"Because KRAS is such an important protein involved in so many cellular processes, resistance to these medications happens quickly and is quite common, since there are a lot of overlapping pathways that interact with KRAS," explained Jane Healy, vice president and head of oncology early development at Merck Research Laboratories. This understanding was pivotal in shaping Merck’s strategy for calderasib. Instead of solely chasing maximal single-agent potency, the company focused on creating an inhibitor that could integrate seamlessly into multi-drug regimens, thereby disrupting multiple resistance pathways simultaneously.
Calderasib’s Design Philosophy: Specificity and Synergy
Merck’s objective with calderasib was to mitigate the rapid emergence of resistance seen with earlier agents while maximizing therapeutic synergy. The design prioritized high specificity for the mutant KRAS G12C protein, minimizing off-target interactions with the wild-type KRAS and thereby reducing potential toxicity. This selectivity is crucial for combination therapies, as it allows for the introduction of additional agents without an unacceptable increase in adverse events.
The core of calderasib’s innovation lies in its capacity for combinability. By designing a drug that is potent yet well-tolerated and specific, Merck aims to create a foundational therapy that can be layered with other agents to block compensatory pathways that cancer cells often exploit to circumvent single-agent inhibition. This approach acknowledges the complex, heterogeneous nature of cancer and the adaptive strategies employed by tumor cells.
Tracking Therapeutic Response Through Liquid Biopsies: The Role of VAF
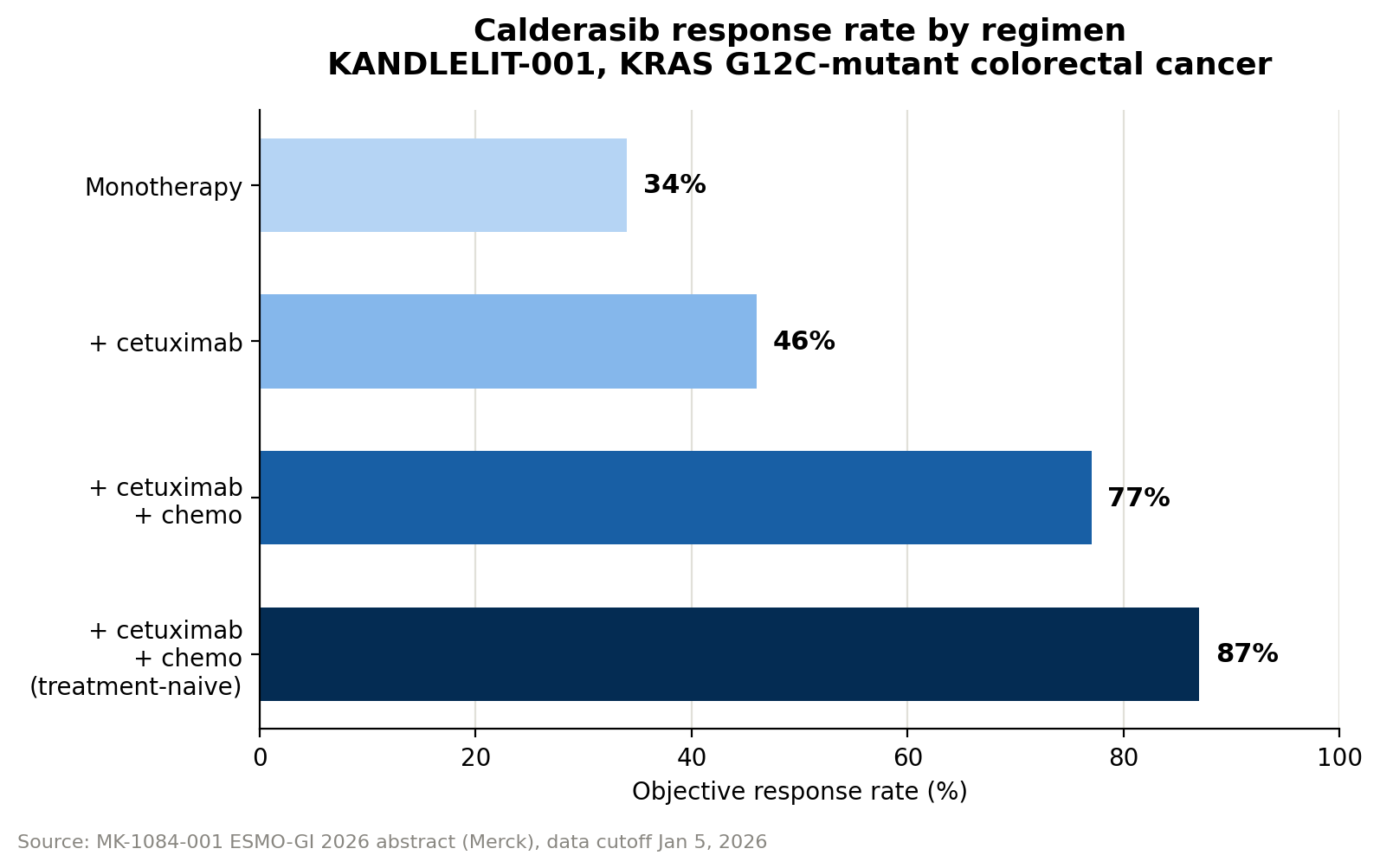
A key component of calderasib’s development strategy involves advanced biomarker tracking, particularly through the use of circulating tumor DNA (ctDNA) and variant allele fraction (VAF). Researchers in the KANDLELIT-001 Phase 1 trial utilized blood draws to collect ctDNA, which comprises fragments of tumor DNA shed into the bloodstream. By measuring the fraction of ctDNA carrying the KRAS G12C mutation – the variant allele fraction – investigators could quantitatively assess the drug’s impact on tumor burden.
VAF serves as a highly sensitive and dynamic biomarker for tracking tumor response. A decline in VAF indicates a reduction in mutant tumor cells circulating and shedding DNA, correlating with a positive therapeutic effect. Conversely, a rise in VAF can signal tumor growth or progression, often preceding changes detectable by conventional imaging techniques. This offers the potential for earlier detection of treatment efficacy or, critically, the emergence of resistance.
"If you track the KRAS G12C variant allele fraction over the course of treatment, it declines, and we can track that across all patients in the study," Healy confirmed. "The reduction in variant allele fraction in the blood correlates quite nicely with the responses we’re seeing by imaging." In the monotherapy arms of the KANDLELIT-001 trial, calderasib led to a median VAF reduction of approximately 95%, dropping from 21% at baseline to 1% at week 6, based on an initial analysis of 18 ctDNA-evaluable patients. Healy further noted that this VAF-response correlation extends across the entire study population, including combination arms, with full data expected in upcoming presentations.
The utility of VAF measurement via blood draws presents several advantages over traditional imaging. It is generally faster, less invasive, and potentially more cost-effective. This enables more frequent monitoring of patients between scans, offering a window into tumor dynamics that could facilitate timelier clinical decisions, such as adjusting treatment regimens in response to early signs of resistance. However, it is important to acknowledge that VAF is a relative fraction, not an absolute measure of tumor burden, and its interpretation must consider the overall quantity of ctDNA shed.
Merck’s Precedent-Setting Tumor-Agnostic Development Strategy
Merck’s approach to calderasib also leverages a well-established regulatory strategy: the tumor-agnostic approval pathway. This innovative framework allows drugs to be approved based on the presence of a specific biomarker, regardless of the tumor’s anatomical origin, rather than confining their indication to a particular organ or tissue type. Merck pioneered this strategy with its blockbuster immunotherapy, pembrolizumab (Keytruda).
"Merck actually had the first tumor-agnostic approval for a drug, with pembrolizumab, through our KEYNOTE-158 program… That was the first tumor-agnostic biomarker approval for a drug," Healy recounted. This landmark approval for pembrolizumab was based on microsatellite instability-high (MSI-High) status, a biomarker indicating deficient mismatch repair genes. Patients with MSI-High tumors demonstrated consistently higher response rates across various cancer types, a finding reinforced by retrospective data from confirmatory trials. Pembrolizumab later secured a second tumor-agnostic approval based on tumor mutational burden (TMB), further solidifying this regulatory pathway.
This precedent has paved the way for a more efficient and patient-centric drug development model. Merck is now applying this validated tumor-agnostic approach to calderasib. "We have a study looking at calderasib activity across tumor types – any patient with a KRAS G12C-mutated solid tumor can enroll – taking a biomarker-driven approach rather than a tumor-type-specific one," Healy elaborated. This means that patients whose tumors harbor the KRAS G12C mutation, irrespective of where the cancer originated in the body, may qualify for trials. This strategy underscores a durable philosophy within Merck, emphasizing the treatment of molecular drivers of cancer rather than solely the organ of origin, marking a significant step toward truly personalized medicine. The ultimate success of this approach for calderasib will, of course, depend on the forthcoming clinical data.
Clinical Data Validates the Combinability Thesis
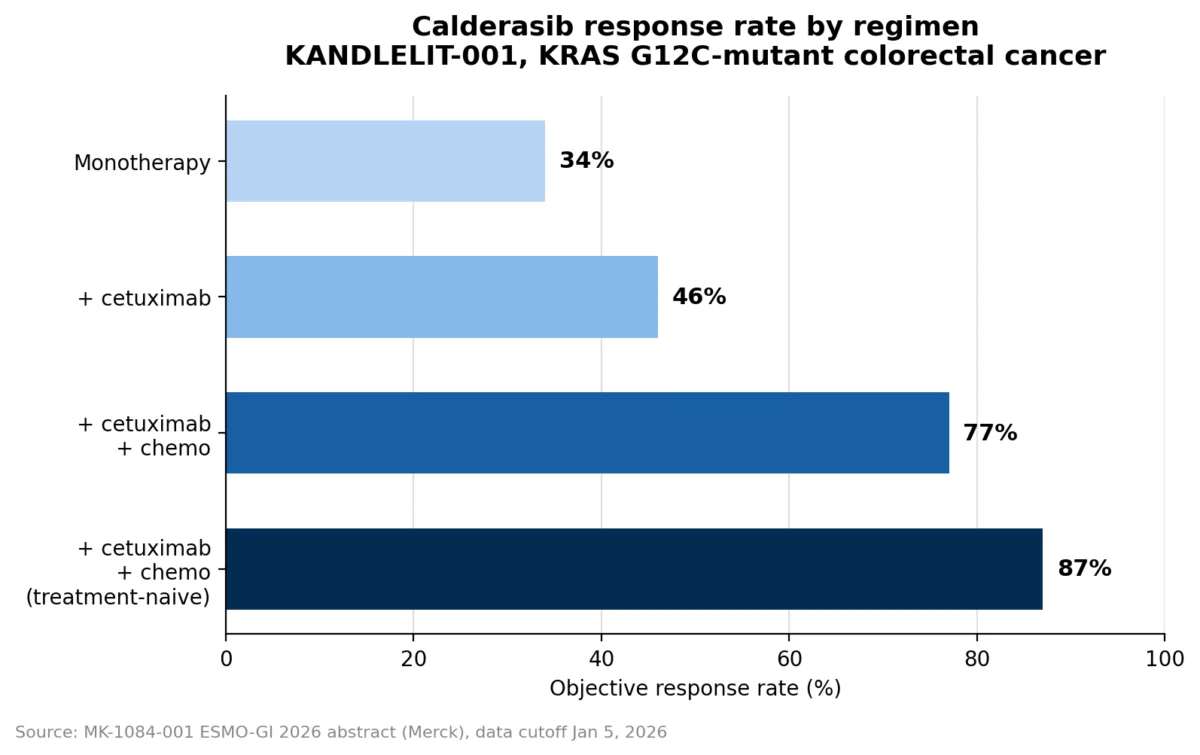
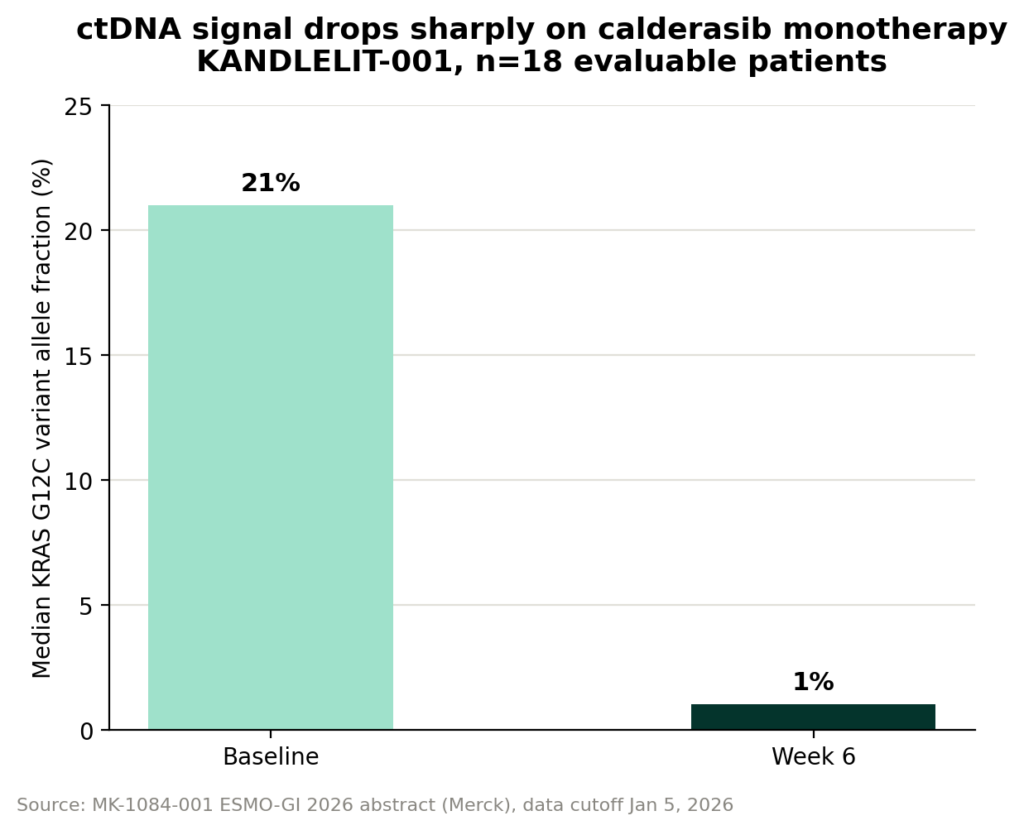
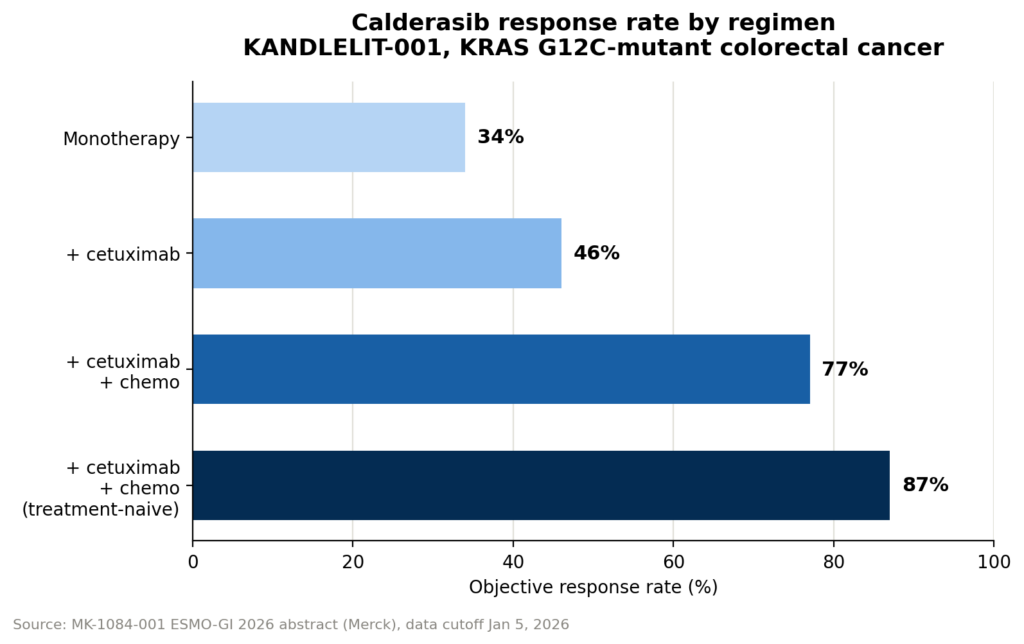
The initial clinical data from the KANDLELIT-001 Phase 1 trial provides compelling evidence for Merck’s combinability thesis. While calderasib as a monotherapy demonstrated an objective response rate (ORR) of 34%, its efficacy significantly improved when combined with other agents.
In combination with cetuximab, an epidermal growth factor receptor (EGFR) inhibitor, the ORR climbed to 46%. The most striking results were observed in the triplet regimen, combining calderasib, cetuximab, and chemotherapy. This combination achieved an impressive ORR of 77%. For patients who had not received prior systemic therapy, the response rate for the triplet regimen was even higher, reaching 87%. These figures strongly support the hypothesis that targeting KRAS G12C in concert with other pathways can dramatically enhance therapeutic outcomes, particularly in previously untreated patients where the disease burden might be more responsive to aggressive intervention.
However, the enhanced efficacy of combination regimens often comes with an increase in adverse events. In the KANDLELIT-001 trial, calderasib monotherapy was generally well-tolerated, with only 9% of patients experiencing grade 3 or 4 drug-related adverse effects. This rate rose to 20% in the doublet arm (calderasib plus cetuximab) and further to 42% in the triplet arm (calderasib, cetuximab, and chemotherapy). While these increases are notable, Healy emphasized that "the combination appears manageable and reflective of the profiles of those individual agents," suggesting that the observed toxicities are largely predictable and consistent with the known side-effect profiles of each component drug.
It is important to contextualize these findings within the limitations of a Phase 1 trial. The dataset is relatively small and non-randomized, meaning the results, while promising, require further validation in larger, controlled studies. The next critical step in this development pathway is the Phase 3 KANDLELIT-012 trial, which will rigorously evaluate calderasib in combination with cetuximab and chemotherapy as a first-line treatment for KRAS G12C-mutant colorectal cancer. This trial will provide definitive evidence regarding the efficacy, safety, and durability of the combination approach in a broader patient population.
Broader Implications and Future Outlook
Merck’s strategic development of calderasib for combinability, coupled with its robust biomarker-driven and tumor-agnostic approach, represents a forward-looking paradigm in oncology. This strategy acknowledges that for many aggressive cancers driven by complex mutations like KRAS G12C, single-agent therapies often face rapid resistance. By designing drugs specifically to be integrated into multi-modal regimens, pharmaceutical companies can potentially achieve deeper and more durable responses, ultimately improving patient outcomes.
The success of calderasib could further cement the importance of liquid biopsies like ctDNA and VAF as routine monitoring tools, offering a less invasive and more dynamic way to track disease progression and treatment response. Moreover, it reinforces the regulatory viability and clinical benefits of the tumor-agnostic approach, potentially accelerating drug development for patients with rare or biomarker-defined cancers across different anatomical sites.
As the oncology landscape continues to evolve, the emphasis on rational combination therapies and precision medicine, guided by sophisticated biomarkers, is becoming paramount. Merck’s calderasib program, with its innovative design and strategic development pathway, stands as a testament to this ongoing transformation, holding significant promise for patients living with KRAS G12C-mutated cancers. The oncology community eagerly awaits the results of the ongoing and future trials, which will determine the full impact of this novel approach.