Recent breakthroughs in genomic sequencing have fundamentally altered our understanding of how the human body ages, revealing that the genetic blueprint we are born with is not the same one we carry into our senior years. A landmark study from Boston Children’s Hospital, published in the journal Cell, has identified an unexpected and profound link between the genetic mutations that cause blood cancers and the progression of Alzheimer’s disease. The research suggests that microglia—the primary immune cells of the brain—accumulate mutations in specific cancer-driving genes that do not result in tumors but instead accelerate neurodegeneration. This discovery challenges long-held assumptions about the isolation of the brain’s immune system and opens a revolutionary door for diagnosing and treating dementia using tools originally developed for oncology.
Led by Christopher Walsh, MD, PhD, Chief of the Division of Genetics and Genomics at Boston Children’s Hospital and an Investigator of the Howard Hughes Medical Institute, the research team focused on the phenomenon of somatic mutations. Unlike germline mutations, which are inherited from parents, somatic mutations occur spontaneously in individual cells throughout a person’s life. While these mutations are the well-known architects of cancer, their role in non-cancerous brain diseases has remained largely mysterious until now.
A Paradigm Shift in Neuro-immunology
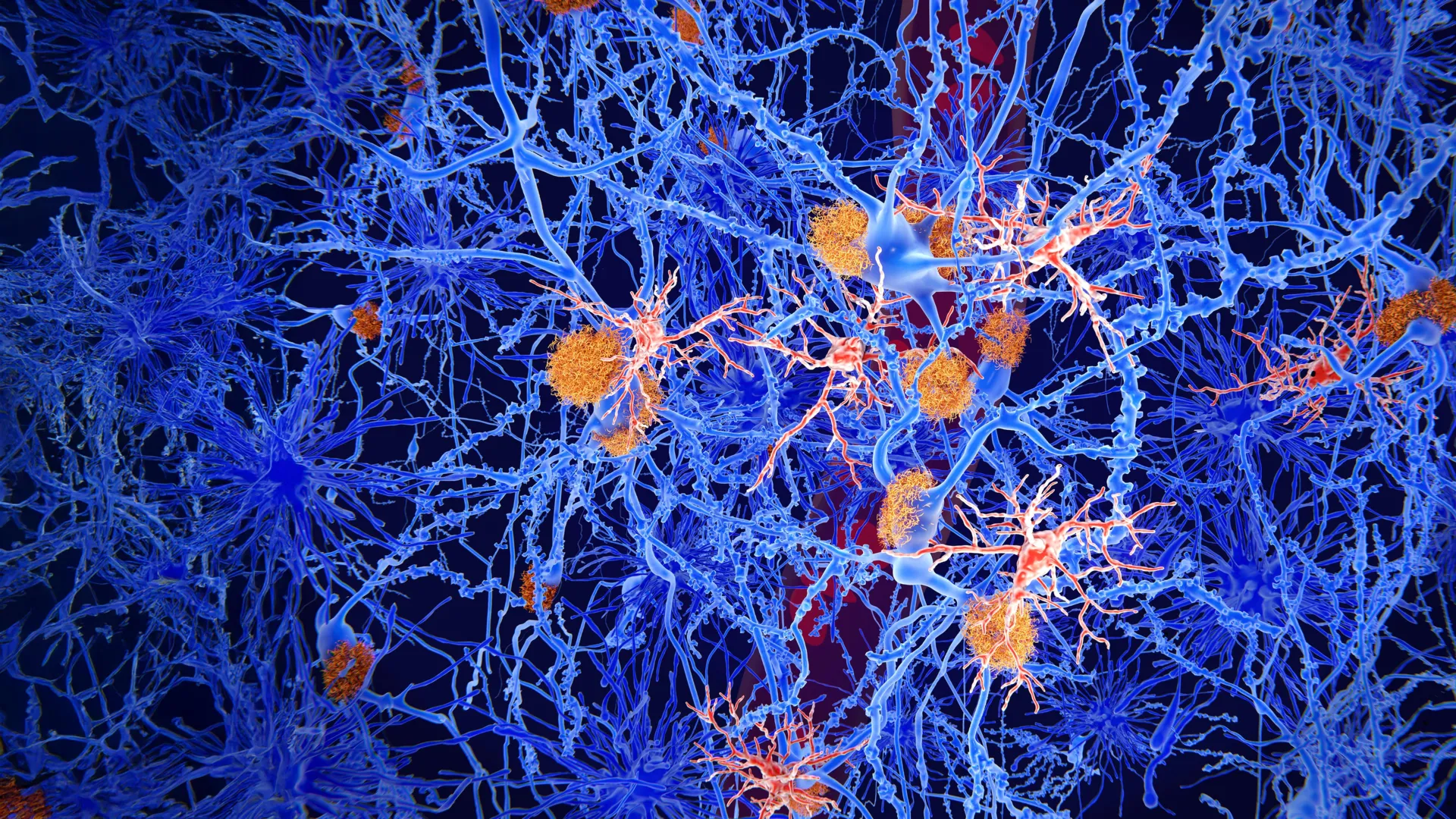
For decades, the scientific community operated under the consensus that the brain was an "immunologically privileged" site, protected by the blood-brain barrier (BBB). This barrier was thought to keep the brain’s immune environment entirely separate from the rest of the body. Microglia were believed to be a self-sustaining population of cells that settled in the brain during embryonic development and remained there for the duration of a person’s life, rarely if ever interacting with immune cells from the bloodstream.
However, the findings from Dr. Walsh’s team suggest a much more dynamic and porous relationship between the blood and the brain. By analyzing the genetic makeup of microglia in patients with Alzheimer’s, the researchers discovered that these cells frequently carry the same mutations found in patients with leukemia and lymphoma.
"We find that to some extent, Alzheimer’s disease is a little like cancer—driven by the same mutations that drive blood cancers," Dr. Walsh stated. This observation is pivotal because it suggests that the inflammatory processes destroying neurons in Alzheimer’s patients may be fueled by "mutant" immune cells that have migrated from the bone marrow into the brain.
Methodology: Deep Sequencing of the Aging Brain
The study involved a rigorous comparative analysis of brain tissue samples. The researchers examined 149 known cancer-driving genes in tissue from 190 individuals diagnosed with Alzheimer’s disease. These were compared against a control group of 121 cognitively healthy individuals.
Using high-depth genetic sequencing, the team looked for "single-letter" DNA changes—point mutations that can alter the function of a protein. The results were striking: the Alzheimer’s-afflicted brains contained a significantly higher burden of these mutations compared to the healthy controls. Most notably, these mutations were not scattered randomly across the genome. Instead, they were concentrated in a specific set of five cancer-driver genes.
This clustering suggests a "selective sweep," a process where cells carrying these specific mutations gain a survival or proliferative advantage. In the context of cancer, this leads to a tumor. In the context of the brain, it leads to a population of "hyper-activated" microglia that may be more aggressive in their inflammatory response, ultimately harming the very neurons they are meant to protect.
The Unexpected Link to the Bloodstream
The most surprising turn in the research occurred when the team decided to cross-reference the brain mutations with the patients’ blood samples. Given the traditional view of the blood-brain barrier, the researchers did not expect to find a match. However, the blood cells of the Alzheimer’s patients carried the exact same cancer-associated mutations as the microglia in their brains.
"It was actually a really unexpected finding that suggests a totally new mechanism for Alzheimer’s disease pathogenesis," said August Yue Huang, PhD, a co-author of the study and professor at Harvard Medical School. "The findings mean that the blood’s immune cells with cancer mutations are likely getting into the brain and contributing to disease."
This phenomenon is closely related to a condition known as Clonal Hematopoiesis of Indeterminate Potential (CHIP). CHIP occurs when a hematopoietic stem cell (a blood-forming cell in the bone marrow) acquires a mutation that allows it to produce a disproportionate number of progeny. While CHIP is common in aging populations and is a known risk factor for cardiovascular disease and leukemia, this study is among the first to provide concrete evidence of its direct involvement in Alzheimer’s pathology.
Chronology of the Pathogenic Process
Based on the data, the researchers have proposed a timeline for how these mutant cells contribute to the decline of the brain:
- Somatic Mutation in Bone Marrow: As an individual ages, a mutation occurs in a blood-forming stem cell in the bone marrow. This mutation often affects genes like DNMT3A or TET2, which are common in blood cancers.
- Clonal Expansion: The mutant stem cell produces a "clone" of immune cells (monocytes) that carry the same mutation. These cells enter the general circulation.
- Barrier Breach: Due to aging, chronic hypertension, or minor injuries, the blood-brain barrier becomes increasingly "leaky." This allows the mutant monocytes to cross from the blood into the brain tissue.
- Transformation: Once inside the brain, these monocytes differentiate into cells that look and act like microglia.
- Inflammatory Feed-Forward Loop: The presence of amyloid-beta plaques and tau tangles—the hallmarks of Alzheimer’s—triggers these microglia to multiply. Because the mutant cells have a competitive advantage, they dominate the population.
- Neurotoxicity: These mutated, "cancer-like" microglia are more prone to producing inflammatory cytokines. This creates a toxic environment that leads to the death of nearby neurons, accelerating the cognitive decline characteristic of Alzheimer’s.
Supporting Data and the APOE4 Factor
To further validate their findings, the research team, including Alice Eunjung Lee, PhD, conducted a follow-up analysis. They investigated whether these blood-borne mutations were simply a byproduct of other risk factors, such as the APOE4 gene, which is the most well-known genetic predictor of Alzheimer’s.
The results, shared in a preprint on bioRxiv, indicated that the presence of cancer-driver mutations in the blood increased the risk of Alzheimer’s disease independently of the APOE4 status. This is a significant finding because it suggests that even individuals without a high-risk genetic profile from birth may develop Alzheimer’s due to the somatic mutations they acquire during their lifetime.
Furthermore, the study noted that the prevalence of these mutations increased with age, correlating with the known epidemiological patterns of Alzheimer’s. The data showed that the "mutational load" in the brain was a better predictor of disease severity in some cases than the absolute density of amyloid plaques, suggesting that the immune response to the plaques might be more damaging than the plaques themselves.
Clinical Implications: From Oncology to Neurology
The implications of this study for the future of Alzheimer’s care are profound, particularly in the realms of diagnostics and therapeutics.
New Diagnostic Frontiers
Currently, diagnosing Alzheimer’s early is difficult, often requiring expensive PET scans or invasive spinal taps to look for protein biomarkers. The discovery of shared mutations in the blood and brain suggests that a simple, non-invasive blood test could be developed. "Because it’s hard to access brain tissue in a living patient, genetic screens using blood samples could be developed to test whether a person carries these mutations," noted Dr. Lee. Such a test could identify individuals at high risk years before cognitive symptoms appear.
Therapeutic Repurposing
Perhaps the most optimistic takeaway is the potential for drug repurposing. The pharmaceutical industry has already spent billions of dollars developing inhibitors for the very pathways identified in this study. If Alzheimer’s is indeed driven by the same mechanisms as certain blood cancers, then existing FDA-approved oncology drugs might be effective in slowing or stopping the progression of dementia.
For example, drugs that target specific kinases or epigenetic regulators in leukemia could theoretically be used to "tame" the hyper-inflammatory mutant microglia in the brain. This could bypass the decades-long development cycle usually required for new Alzheimer’s medications.
Institutional Collaboration and Future Research
This research was a multi-institutional effort, involving the Icahn School of Medicine at Mount Sinai and the Broad Institute of MIT and Harvard. It was supported by the Howard Hughes Medical Institute and the National Institute on Aging, as well as the Somatic Mosaicism Across Human Tissues (SMaHT) consortium.
The SMaHT consortium, funded by the NIH Common Fund, is currently working to map how somatic mutations vary across different tissues in the human body. The Boston Children’s Hospital study serves as a cornerstone for this initiative, proving that mutations in one tissue system (the blood) can have devastating consequences in another (the brain).
Moving forward, the researchers plan to investigate whether specific lifestyle factors or environmental exposures accelerate the accumulation of these mutations. They also aim to conduct clinical trials to see if targeting these mutant immune cells can preserve cognitive function in animal models of Alzheimer’s, with the eventual goal of human trials.
Conclusion: A New Lens on Aging
The study from Dr. Walsh and his colleagues marks a significant shift in the narrative of neurodegenerative disease. By reframing Alzheimer’s not just as a disease of "protein misfolding," but as a disease influenced by "somatic evolution" and "leaky" systemic immunity, the research provides a clearer picture of why the disease is so closely tied to the aging process.
As the global population ages and the burden of Alzheimer’s disease is expected to triple by 2050, these findings offer a much-needed new direction for scientific inquiry. The realization that the tools to fight the brain’s greatest enemy might already exist in the cabinet of the oncologist provides a glimmer of hope for millions of patients and their families worldwide. By bridging the gap between blood and brain, and between cancer and dementia, this research has set the stage for a new era of precision medicine in neurology.