Every single second, the human bone marrow performs a biological feat of staggering proportions, generating millions of new blood and immune cells to sustain the body’s circulatory and defense systems. This relentless cycle of renewal is governed by a sophisticated biological theater known as the hematopoietic niche. In this specialized environment, hematopoietic stem cells (HSCs) reside in a state of carefully regulated balance, supported by an intricate scaffolding of stromal cells and a constant stream of biochemical signals. However, as the human body ages, this once-harmonious ecosystem begins to fracture. New research led by an international consortium of scientists has revealed that the roots of blood-related malignancies may not lie solely within mutated stem cells themselves, but rather in a profound and early remodeling of the surrounding bone marrow microenvironment.
For decades, hematology research focused primarily on the genetic mutations within stem cells that lead to leukemia and other blood disorders. Yet, the question of why some mutated cells remain dormant while others aggressively expand has remained one of the most significant mysteries in oncology. A groundbreaking study, co-led by Professor Judith Zaugg of EMBL and the University of Basel, and Dr. Borhane Guezguez of University Medical Center (UMC) Mainz, has now mapped the hidden cellular shifts that occur long before clinical symptoms manifest. By analyzing the bone marrow of healthy individuals, those with Clonal Hematopoiesis of Indeterminate Potential (CHIP), and patients with Myelodysplastic Syndrome (MDS), the team has identified a dominant inflammatory loop that fundamentally alters the "soil" in which blood cells grow.
The Rise of CHIP and the Path to Malignancy
The transition from healthy aging to blood cancer is often a decades-long process. It frequently begins with a condition known as Clonal Hematopoiesis of Indeterminate Potential, or CHIP. This phenomenon occurs when a single mutated hematopoietic stem cell gains a competitive advantage and begins to produce a disproportionate share of the body’s blood cells. While CHIP is not a cancer in itself—most individuals with the condition have normal blood counts and no outward symptoms—it serves as a critical harbinger of future health risks.
Statistical data indicates that CHIP is a hallmark of the aging process. It is detected in approximately 10% to 20% of adults over the age of 60, and its prevalence surges to nearly 30% in those over the age of 80. While the condition was once thought to be a benign consequence of aging, clinical data now paints a more concerning picture. Individuals with CHIP face a tenfold increase in the risk of developing hematologic malignancies. Perhaps more surprisingly, the condition is also linked to a doubling of the likelihood of cardiovascular disease and a significantly higher rate of early mortality, likely due to the systemic inflammation generated by mutated immune cells.
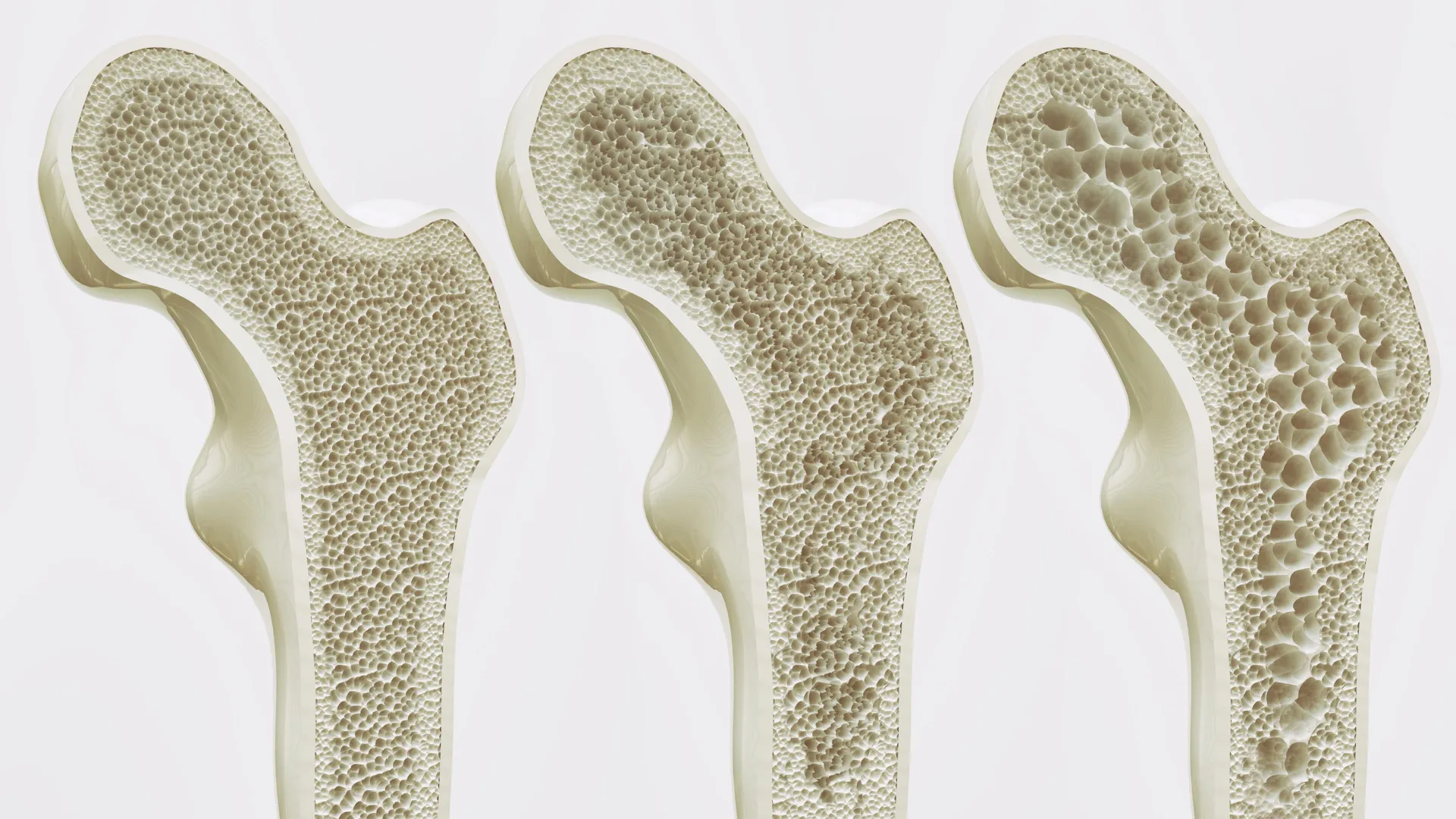
When CHIP progresses, it often evolves into Myelodysplastic Syndrome (MDS). MDS is a group of diverse bone marrow disorders characterized by "ineffective" hematopoiesis, where the marrow produces misshapen and dysfunctional blood cells. For patients over the age of 70, the incidence of MDS rises to 20 per 100,000 individuals. The prognosis for MDS is often grim; roughly 30% of cases advance to Acute Myeloid Leukemia (AML), an aggressive cancer with high mortality rates. Understanding the triggers that push a patient from the relatively stable state of CHIP to the life-threatening state of MDS or AML is the central focus of modern hematological research.
Mapping the Bone Marrow Landscape
To investigate these triggers, the research team conducted an exhaustive molecular and spatial analysis of human bone marrow samples. This effort was supported by the BoHemE cohort study, a collaborative initiative involving Uwe Platzbecker at the National Center for Tumor Diseases (NCT) Dresden. The researchers employed a multi-omic approach, combining single-cell RNA sequencing, advanced biopsy imaging, proteomics, and sophisticated co-culture models to create a high-definition map of the bone marrow niche.
The methodology allowed the team to observe the bone marrow at an unprecedented level of detail. One of the primary challenges in studying these disorders is the difficulty of distinguishing mutated cells from healthy ones within a single tissue sample. To overcome this, the researchers utilized a new computational tool called SpliceUp. Developed by co-lead author Maksim Kholmatov in collaboration with experts from the Karolinska Institute, SpliceUp identifies mutated cells by detecting abnormal RNA-splicing patterns that are characteristic of MDS. This allowed the scientists to separate the "signals" sent by mutated cells from the "noise" of the surrounding healthy tissue, leading to a startling discovery.
The Discovery of Inflammatory Stromal Cells (iMSCs)
The study’s most significant finding was the identification of a cellular shift that begins during the CHIP stage, well before MDS is clinically diagnosed. In a healthy bone marrow niche, mesenchymal stromal cells (MSCs) provide the structural and biochemical support necessary for stem cell health. However, the researchers found that in individuals with CHIP and MDS, these supportive cells are gradually replaced by a new, pathological population: inflammatory stromal cells (iMSCs).
"I was surprised to observe such pronounced remodeling of the bone marrow microenvironment already in individuals with CHIP," noted Professor Judith Zaugg. These iMSCs represent a fundamental departure from normal physiology. Instead of nurturing stem cells, iMSCs produce high volumes of interferon-induced cytokines and chemokines. These pro-inflammatory molecules act as a beacon, attracting and activating interferon-responsive T cells.
This interaction creates what the researchers describe as a "feed-forward loop." The T cells, once activated, further stimulate the stromal cells to maintain their inflammatory state. This chronic inflammatory environment disrupts the normal production of blood cells and causes physical changes to the marrow’s vascular structure. Crucially, the researchers found that this inflammatory network becomes the dominant feature of the bone marrow, effectively "crowding out" the regenerative structures that the body needs to maintain healthy blood production.
Disruption of Essential Signaling Pathways
Beyond the presence of inflammation, the study highlighted a critical failure in cellular communication. In a healthy marrow, a signaling molecule known as CXCL12 is essential for telling blood cells where to settle and mature within the bone marrow. The researchers observed that in MDS, the mutated stem cells lose the ability to trigger stromal cells to produce this vital signal.
"This failure may help explain why the bone marrow stops working properly," said Karin Prummel, co-lead author and EMBL postdoc. Without the correct spatial cues provided by CXCL12, the hematopoietic process becomes disorganized. This lack of "homing" signals contributes to the marrow’s inability to produce mature, functional blood cells, leading to the cytopenias (low blood counts) that characterize MDS.
Interestingly, the data suggested that the mutated hematopoietic cells do not necessarily "cause" this inflammation through direct action. Instead, the entire ecosystem—the stromal cells and the immune T cells—appears to shift into a pro-inflammatory state that then favors the expansion of mutated clones. This suggests that the bone marrow microenvironment is not a passive bystander but an active driver of disease progression.
The Concept of ‘Inflammaging’ and Systemic Health
The findings of this study extend far beyond the realm of blood cancer, contributing to a growing body of evidence regarding "inflammaging." This term refers to the low-grade, chronic, systemic inflammation that characterizes biological aging. Inflammaging is increasingly recognized as a root cause of many age-related pathologies, including neurodegenerative diseases, metabolic disorders, and cardiovascular dysfunction.
The bone marrow is now being viewed as a central hub for inflammaging. Because the marrow produces the immune cells that circulate throughout the entire body, any inflammatory shift within the marrow niche has systemic consequences. The pro-inflammatory T cells and cytokines identified in this study do not remain confined to the bone marrow; they enter the bloodstream, potentially contributing to the arterial inflammation and plaque instability that explain the high cardiovascular risk seen in CHIP patients.
By demonstrating how the interaction between immune and stromal cells drives these changes, the study provides a template for understanding inflammatory remodeling in other tissues. It suggests that treating the "environment" may be just as important as treating the "disease" itself.
Future Directions: Prevention and Therapeutic Intervention
The realization that the microenvironment shapes the earliest stages of malignancy opens new doors for preventive medicine. Currently, medical practice for CHIP is largely "watchful waiting," as there are few established therapies to prevent the transition to MDS. However, this research points toward several potential interventions:
- Anti-inflammatory Therapies: The use of existing anti-inflammatory drugs or new therapies targeting interferon signaling could potentially suppress the iMSC population and break the inflammatory loop, preserving marrow function in older adults.
- Early Biomarkers: The specific molecular signatures of iMSCs and interferon-responsive T cells could serve as early-warning biomarkers. Identifying these signatures in routine biopsies could help clinicians pinpoint which CHIP patients are at the highest risk of progressing to leukemia.
- Niche-Targeted Treatments: Future treatments might focus on "rehabilitating" the bone marrow niche. By restoring the production of signals like CXCL12, it may be possible to improve blood cell production even in the presence of mutated stem cells.
- Improving Transplant Success: The study also has implications for bone marrow transplants. If the "niche" retains a memory of the disease even after malignant cells are removed, it may explain why some transplants fail. Understanding how to "reset" the niche could improve outcomes for transplant recipients.
"Our findings reveal that the bone marrow microenvironment actively shapes the earliest stages of malignant evolution," stated Dr. Borhane Guezguez. "Understanding how stromal and immune cells interact provides a foundation for preventive therapies that intercept disease progression before leukemia develops."
This research was published in Nature Communications alongside a complementary study led by Marc Raaijmakers from the Erasmus MC Cancer Institute. Together, these works provide the most comprehensive view to date of the inflammatory remodeling that defines the early phases of bone marrow disease. As the global population ages, the ability to intercept these processes before they turn fatal will become a cornerstone of 21st-century hematology, shifting the focus from treating advanced cancer to maintaining the long-term health of the human bone marrow factory.