The human bone marrow functions as a biological factory of staggering proportions, generating millions of new blood and immune cells every second. This relentless cycle of renewal is governed by a sophisticated ecosystem where hematopoietic stem cells (HSCs) reside within specialized "niches." These niches are composed of supportive stromal cells, blood vessels, and signaling molecules that dictate when a stem cell should remain dormant, self-renew, or differentiate into specialized cells like oxygen-carrying erythrocytes or infection-fighting leukocytes. However, as the human body ages, this equilibrium begins to falter. New research led by an international consortium of scientists has revealed that the "soil" of the bone marrow—the microenvironment—undergoes profound inflammatory remodeling long before the onset of clinical disease, providing a fertile ground for the expansion of mutated cells and the eventual development of blood cancers.
The Silent Rise of Clonal Hematopoiesis
As individuals age, they frequently acquire somatic mutations in their hematopoietic stem cells. When a mutated stem cell gains a fitness advantage and begins to produce a disproportionate share of the body’s blood cells, the condition is known as clonal hematopoiesis of indeterminate potential (CHIP). While CHIP is not a cancer in itself, it represents a significant pre-malignant state. Statistics indicate that CHIP is present in approximately 10 to 20% of adults over the age of 60, and its prevalence surges to nearly 30% in those over 80.
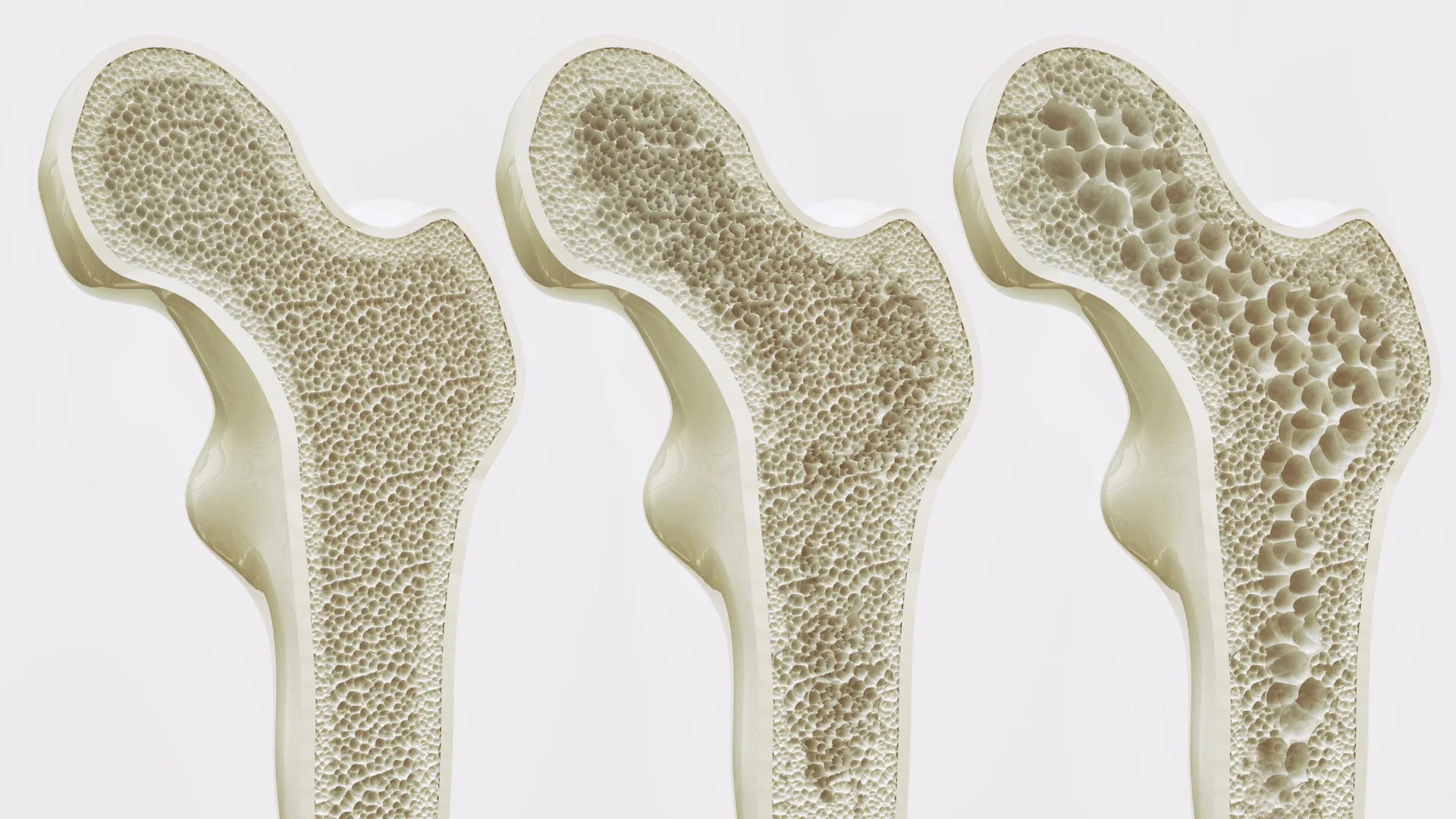
For years, CHIP was viewed as a relatively benign consequence of aging. However, recent epidemiological data has painted a more concerning picture. Individuals with CHIP face a tenfold increase in the risk of developing hematologic malignancies. Perhaps more surprisingly, the condition is linked to a twofold increase in the risk of cardiovascular diseases, such as myocardial infarction and stroke, and a higher rate of all-cause mortality. The transition from CHIP to more severe disorders, such as myelodysplastic syndrome (MDS), marks a critical clinical threshold. MDS is characterized by "ineffective hematopoiesis," where the bone marrow produces malformed or dysfunctional blood cells. With an incidence rate of 20 per 100,000 in adults over 70, MDS is a precursor to acute myeloid leukemia (AML) in roughly 30% of cases—a progression that often carries a grim prognosis.
Mapping the Bone Marrow Niche at Single-Cell Resolution
To investigate why some mutated clones remain dormant while others progress to malignancy, a research team co-led by Judith Zaugg of EMBL and the University of Basel, and Borhane Guezguez from UMC Mainz, conducted a comprehensive spatial and molecular audit of the bone marrow. The study utilized samples from the BoHemE cohort, a specialized group of patients and healthy donors managed in collaboration with the National Center for Tumor Diseases (NCT) Dresden.
The methodology employed was multi-omic and highly granular. The team integrated single-cell RNA sequencing, high-resolution biopsy imaging, and proteomics to visualize the bone marrow’s architecture. This allowed them to move beyond a simple tally of cell types and instead examine the "conversations" happening between cells. One of the most significant hurdles in studying MDS and CHIP is the difficulty of distinguishing mutated stem cells from healthy ones within a single sample. To solve this, the researchers used a computational tool called SpliceUp. Developed by Maksim Kholmatov, an EMBL alumnus, in collaboration with the Karolinska Institute, SpliceUp identifies mutated cells by detecting abnormal RNA-splicing patterns—a hallmark of many hematopoietic mutations. This technological breakthrough allowed the team to observe how mutated cells interact with their surroundings compared to their healthy counterparts.
The Shift to an Inflammatory Stroma
The most striking discovery of the study was the identification of a massive cellular shift within the bone marrow’s support structure. In healthy marrow, mesenchymal stromal cells (MSCs) provide the necessary signals to maintain stem cell health. However, in patients with CHIP and MDS, these healthy MSCs are gradually replaced by a population the researchers termed inflammatory mesenchymal stromal cells (iMSCs).
"I was surprised to observe such pronounced remodeling of the bone marrow microenvironment already in individuals with CHIP," noted Judith Zaugg. The research revealed that these iMSCs are not passive bystanders. Instead, they act as inflammatory hubs, secreting high levels of interferon-induced cytokines and chemokines. These chemical signals act as a beacon for T cells, specifically those responsive to interferon. Once these T cells enter the marrow, they release further inflammatory signals, creating a self-sustaining "feed-forward" loop. This chronic inflammatory state disrupts the marrow’s normal regenerative capacity and alters the vascular network, effectively poisoning the "soil" in which blood cells grow.
The Failure of Cellular Communication
A key finding of the research was the breakdown of the CXCL12 signaling pathway. In a healthy environment, stromal cells produce CXCL12, a protein that acts as a homing signal, telling blood cells where to settle and mature within the bone marrow. The study found that MDS stem cells are unable to trigger the production of this vital signal in stromal cells.
"This failure may help explain why the bone marrow stops working properly," explained Karin Prummel, a co-lead author and EMBL postdoc. Without the correct spatial cues, the production of blood cells becomes disorganized and inefficient. Interestingly, the researchers found that the inflammatory response was not necessarily a direct reaction to the mutated cells themselves. Instead, the inflammation appeared to be a systemic shift in the microenvironment that precedes or facilitates the dominance of mutated clones. This suggests that the "niche" may be just as responsible for disease progression as the mutations within the stem cells.
The Concept of ‘Inflammaging’ and Systemic Impact
The study’s findings contribute significantly to the burgeoning field of "inflammaging"—the theory that chronic, low-grade inflammation is a primary driver of aging and age-related diseases. The bone marrow, traditionally viewed solely as a site for blood production, is now being recognized as a central player in systemic aging. The inflammatory environment identified in the marrow does not remain localized; the cytokines and activated immune cells produced there can enter the general circulation, contributing to the systemic inflammation linked to metabolic disorders and heart disease.
This systemic connection explains why CHIP is a risk factor for more than just leukemia. The same inflammatory processes that allow a mutated blood clone to expand also accelerate the buildup of arterial plaque (atherosclerosis), linking bone marrow health directly to cardiovascular longevity.
Implications for Future Therapies and Prevention
The identification of iMSCs and interferon-responsive T cells as key drivers of marrow decay opens several new avenues for clinical intervention. Current treatments for MDS and AML often focus on eradicating the malignant cells through chemotherapy or targeted inhibitors. However, if the underlying bone marrow niche remains inflammatory, the risk of relapse remains high because the "soil" is still primed for disease.
- Anti-inflammatory Interventions: The study suggests that existing anti-inflammatory drugs or therapies targeting interferon signaling could be repurposed to preserve bone marrow function in older adults. By "cooling down" the niche, it may be possible to prevent the expansion of mutated CHIP clones before they transition into MDS.
- Early Biomarkers: The specific molecular signatures of iMSCs could serve as early warning signs. Routine marrow biopsies or even advanced blood tests could one day screen for these inflammatory markers, identifying high-risk individuals decades before leukemia develops.
- Improving Transplant Outcomes: Stem cell transplantation is a common treatment for blood cancers, but it often fails if the recipient’s bone marrow niche is too damaged. "We are now investigating to what extent the niche retains a ‘memory’ of disease," Zaugg said. Understanding this memory could lead to "niche-priming" therapies that prepare the bone marrow to receive and support new, healthy stem cells more effectively.
A Growing Consensus in Hematology
The findings of the EMBL and UMC Mainz team were published alongside a complementary study in Nature Communications led by Marc Raaijmakers of the Erasmus MC Cancer Institute. Together, these two studies provide a robust, multi-perspective view of how the bone marrow microenvironment evolves during the early stages of malignancy. The convergence of data from different cohorts and research teams reinforces the conclusion that the microenvironment is a primary actor, rather than a secondary victim, in the development of blood disorders.
The research was a global effort, involving institutions from Germany, Switzerland, Sweden, France, and the United States. Funding was provided by various prestigious bodies, including the European Research Council (ERC), the Swiss National Foundation, and the José Carreras Leukaemia Foundation.
As the global population ages, the burden of CHIP, MDS, and AML is expected to rise. This research marks a paradigm shift in how hematologists and oncologists view these conditions. By shifting the focus from the "seed" (the mutated cell) to the "soil" (the inflammatory niche), science is moving closer to a future where blood cancers can be intercepted and prevented rather than just treated in their advanced, often fatal, stages. The discovery that the bone marrow microenvironment actively shapes the earliest stages of malignant evolution provides a foundational roadmap for the next generation of preventive medicine.