The global healthcare landscape is currently grappling with a silent but pervasive skeletal condition known as osteopenia, which now affects approximately 40% of the adult population worldwide. Defined as the loss of bone mineral density (BMD) that is lower than normal but not yet classified as osteoporosis, osteopenia serves as a critical clinical precursor to more severe skeletal fragility. In the United Kingdom alone, health authorities estimate that more than 500,000 fragility fractures occur annually, a statistic directly linked to the diminishing bone health of an aging population. Despite its high prevalence, osteopenia remains frequently under-diagnosed because it rarely presents with overt symptoms until a bone actually breaks. This "silent" progression has led public health experts to advocate for earlier screening and more robust lifestyle interventions to mitigate a looming crisis in geriatric care and surgical demand.
The Biological Mechanism of Bone Remodeling
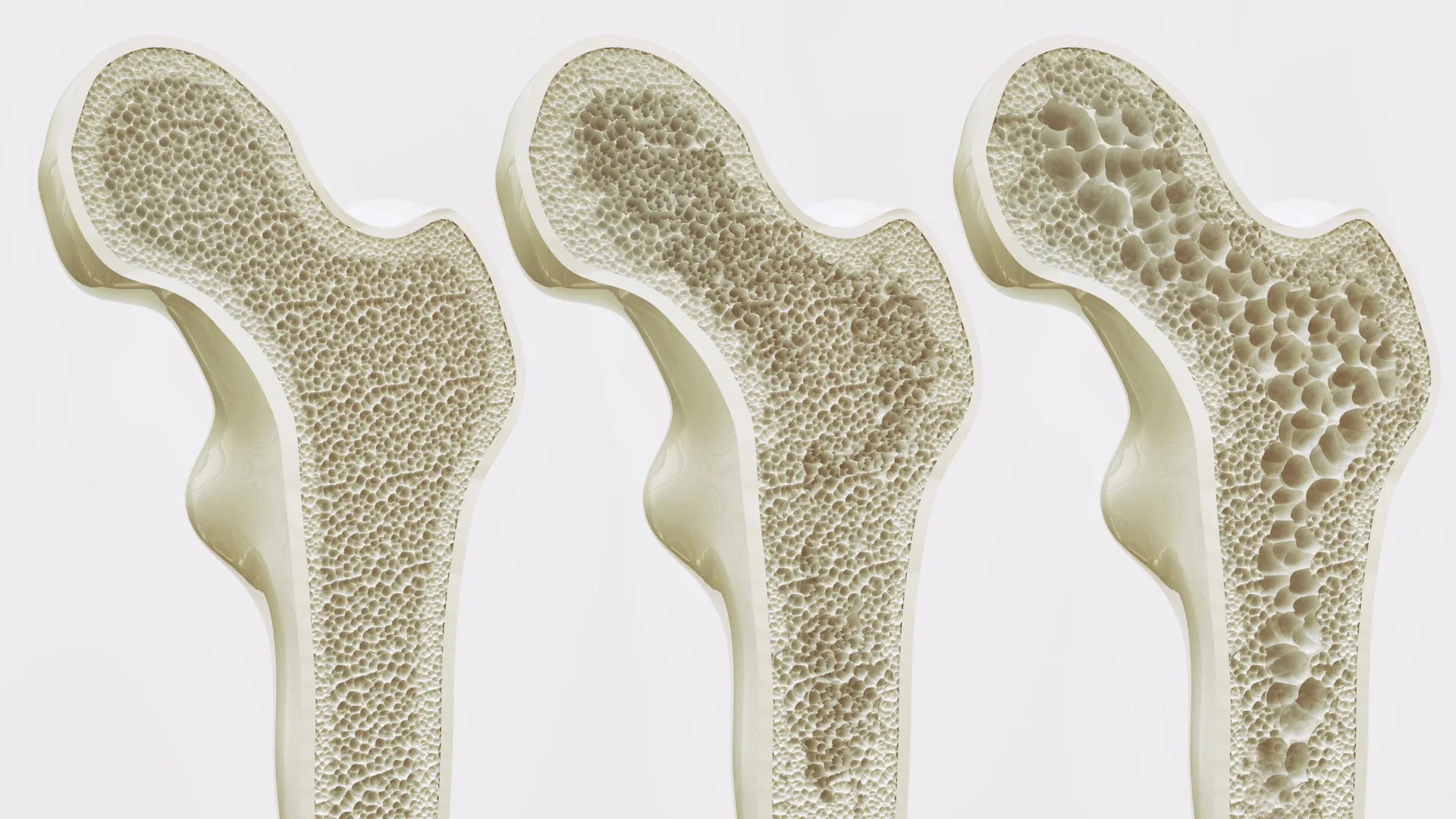
To understand the trajectory of osteopenia, one must look at the microscopic processes governing human skeletal integrity. Bone is not a static structure but a dynamic, living tissue that undergoes a continuous cycle of renewal known as bone remodeling. This process involves two primary actions: resorption, where specialized cells called osteoclasts break down old or damaged bone tissue, and formation, where osteoblasts deposit new bone mineral.
In a healthy young adult, these two processes are meticulously balanced. During childhood and adolescence, bone formation significantly outpaces resorption, leading to a steady increase in skeletal mass. Most individuals reach their "peak bone mass" between their mid-20s and early-30s. This peak serves as a person’s "bone bank," providing the reservoir of mineral density they will rely on for the rest of their lives. However, once this peak is surpassed, the biological equilibrium shifts. Gradually, the rate of bone resorption begins to exceed the rate of formation. Over decades, this imbalance leads to a thinning of the bone matrix and a reduction in mineral content, culminating in the diagnostic state of osteopenia.
Primary Risk Factors and the Menopause Transition
While aging is the universal driver of bone loss, certain demographics face a disproportionately high risk. Postmenopausal women represent the largest cohort affected by osteopenia due to the precipitous decline in estrogen levels. Estrogen plays a vital protective role in skeletal health by inhibiting the activity of osteoclasts. When estrogen levels drop during and after menopause, the natural "brakes" on bone breakdown are removed, leading to a rapid acceleration of bone loss.
Clinical data suggests that approximately one in two women over the age of 50 will suffer a fragility fracture in their remaining lifetime. The vulnerability of this demographic has prompted organizations like the Royal Osteoporosis Society (ROS) to call for more comprehensive bone health assessments during routine menopause consultations. Beyond hormonal changes, other non-modifiable risk factors include genetics, ethnicity (with Caucasian and Asian populations showing higher susceptibility), and small body frames, which often correlate with lower initial peak bone mass.
Secondary Influences: Lifestyle and Medical Comorbidities
The progression of osteopenia is not dictated solely by age and hormones; lifestyle choices and secondary health conditions play a decisive role in skeletal degradation. Chronic physical inactivity is a leading contributor to weakened bones, as the skeleton requires mechanical "loading" to signal the body to maintain bone density. Conversely, habits such as smoking and excessive alcohol consumption have been shown to interfere with calcium absorption and osteoblast function, further compromising the structural integrity of the ribs, hips, and spine.
Dietary deficiencies also remain a significant concern in the developed world. Calcium is the primary building block of bone tissue, but its absorption is dependent on adequate levels of Vitamin D. In northern latitudes, such as the UK and parts of North America, Vitamin D deficiency is a seasonal certainty for many, necessitating supplementation to prevent the body from "leaching" calcium from the bones to maintain vital blood-calcium levels.
Furthermore, certain medical interventions can inadvertently damage bone health. Long-term use of corticosteroids (such as prednisolone for asthma or arthritis) is a well-documented cause of secondary osteopenia. Conditions that cause malabsorption, such as Crohn’s disease, ulcerative colitis, or coeliac disease, can also deprive the body of the nutrients required for bone maintenance, making these patients high-priority candidates for early BMD screening.
Diagnostic Standards and the T-Score System
The clinical "gold standard" for identifying osteopenia is the Dual-energy X-ray Absorptiometry (DXA) scan. This non-invasive, low-dose X-ray measures the mineral content of specific areas, typically the hip and the lumbar spine. The results are converted into a "T-score," which represents the number of standard deviations a patient’s bone density sits above or below that of a healthy 30-year-old of the same sex.

According to the World Health Organization (WHO) diagnostic criteria:
- Normal: T-score of -1.0 or higher.
- Osteopenia: T-score between -1.0 and -2.5.
- Osteoporosis: T-score of -2.5 or lower.
A T-score in the osteopenia range serves as a vital clinical warning. It indicates that while the bones are not yet "porous" (the literal meaning of osteoporosis), they have lost enough density to be at an increased risk of fracture. To refine treatment decisions, clinicians often use the FRAX (Fracture Risk Assessment Tool), which calculates a patient’s 10-year probability of a major osteoporotic fracture by combining BMD data with other risk factors like smoking history, family history of hip fractures, and alcohol intake.
Clinical Management and the Role of Physical Activity
Managing osteopenia requires a multi-pronged approach aimed at stabilizing bone density and preventing the transition to osteoporosis. For many patients, the first line of defense is specialized exercise. Weight-bearing physical activity—where the bones support the weight of the body—is essential. Activities such as brisk walking, jogging, and dancing create small amounts of stress on the bones, which in turn stimulates osteoblasts to produce more bone tissue.
Resistance training, including weightlifting or using resistance bands, is equally critical. By strengthening the muscles surrounding the bones, individuals can improve their overall stability and reduce the likelihood of falls. Balance-focused exercises, such as Tai Chi, have gained significant clinical endorsement. Research indicates that Tai Chi not only helps maintain BMD in the hips and spine but significantly reduces fall risk among the elderly, thereby preventing the "fall-fracture-hospitalization" cycle that often leads to a decline in quality of life.
Nutritional Interventions and Pharmacotherapy
Nutrition remains a cornerstone of bone health management. The NHS recommends that adults consume approximately 700mg to 1,000mg of calcium daily, ideally through diet. Dairy products, leafy greens (like kale and collards), and fortified cereals are primary sources. However, for those with osteopenia, clinicians may prescribe calcium and Vitamin D3 supplements to ensure the skeletal system has a constant supply of raw materials for repair.
While not everyone with osteopenia requires medication, pharmacotherapy is considered for high-risk individuals. Antiresorptive medications, such as bisphosphonates (e.g., alendronate), work by slowing down the cells that break down bone. Though more commonly associated with osteoporosis treatment, recent longitudinal studies suggest that high-risk osteopenic patients—particularly those who have already suffered a minor "fragility fracture"—benefit significantly from early pharmaceutical intervention to prevent further degradation.
The Socio-Economic Impact and Public Health Analysis
The rise in osteopenia cases presents a staggering economic challenge for global healthcare systems. In the UK, the cost of treating fragility fractures is estimated to exceed £4 billion annually, a figure expected to rise as the "baby boomer" generation reaches advanced age. Beyond the financial cost, the human cost is profound; hip fractures, in particular, are associated with high mortality rates and a permanent loss of independence for many seniors.
Analysis of current trends suggests that the medical community is shifting toward a "preventative" rather than "reactive" model. By identifying osteopenia in a patient’s 50s or 60s, healthcare providers can implement lifestyle changes that potentially add decades of skeletal health. This shift is viewed by health economists as a necessary evolution to ensure the sustainability of geriatric care.
A Lifespan Perspective on Prevention
Ultimately, the fight against osteopenia is a lifelong endeavor. Bone health is the cumulative result of decades of nutrition, activity, and hormonal balance. Public health experts emphasize that while osteopenia is a warning sign, it is not an inevitable sentence of decline. Evidence suggests that with targeted lifestyle adjustments, some patients can not only stop bone loss but actually improve their T-scores over time.
As the global population ages, the "silent" threat of osteopenia must be met with loud and clear public health messaging. Awareness of peak bone mass in youth, combined with rigorous screening for postmenopausal women and elderly men, remains the most effective strategy for reducing the global burden of fractures. By treating osteopenia as a critical point of intervention rather than a mild condition, society can better protect the mobility and dignity of its aging members. Maintaining skeletal strength is not merely a medical goal but a fundamental component of healthy aging, requiring a commitment to "bone-friendly" habits that span from the playground to the retirement home.